
Dec 28, 2018
Another exciting issue of European Neurological Review is now released, highlighting new advances in the field of Neurology, as well as featuring SAFE’s information about the Stroke Action Plan for Europe.
 We find one of the case reports from this issue particularly interesting, covering a rare syndrome that can occur in persons with an ischaemic stroke.
We find one of the case reports from this issue particularly interesting, covering a rare syndrome that can occur in persons with an ischaemic stroke.
Charles Bonnet syndrome (CBS) is characterised by the presence of visual hallucinations (VH) and visual sensory deprivation in individuals with preserved cognitive status and without a history of psychiatric illness. CBS is a rare, underdiagnosed and under-recognised syndrome, which was first described in 1769 by Charles Bonnet, who observed this phenomenon in his grandfather.
The prevalence of CBS is not consistent between authors. Some studies have stated that 0.47% of the general population suffer from CBS – this number can increase to around 15–30% when referring to patients with visual impairment. The disparity in CBS prevalence can be explained by the absence of clear diagnostic criteria, the necessity of different specialties to recognise or exclude other disorders and the incapability of patients to express the symptoms.2,3 CBS usually occurs in elderly people with compromised visual function and can be a rare manifestation of an injured visual pathway. Secondary lesions to multiple sclerosis, ischaemic stroke, temporal arteritis and meningiomas can explain the syndrome. This case report presents a variant of CBS as consequence of an ischaemic stroke in left occipitotemporal regions. In our view, the particularities and variations of CBS should be widespread, as it can be the only manifestation of an ischaemic stroke that requires appropriate and immediate management.
You can read the full case report here and you can find more articles from the latest issue here.
Dec 21, 2018
Oruen – The CNS Journal has now been published online. In this issue you can find the SAFE special report on stroke prevention project and Stroke Action Plan for Europe advert. SAFE is also mentioned in the two ANGELS articles.
The current issue also brings you the following reviewed articles:
Clinical Outcomes and Work Flow Optimisation with Pipeline System and Shield Technology (Istvan Szikora, Saleh Lamin, Mohamed Aggour)
Innovations in Endovascular Treatment of Acute Ischemic Stroke and Cerebral Aneurysms (Hannes A. Deutschmann, Marc Ribo, Mathieu Sanchez)
The ANGELS Initiative: More and better Stroke-ready Hospitals across the globe (Rob Goodwin)
Improving stroke care across the world: The Angels Initiative (Valeria Caso, Magd Fouad Zakaria, Ales Tomek, Robert Mikulik, Sheila Cristina Ouriques Martins, Thang Huy Nguyen, Anastasia Rossouw)
Stroke Prevention in atrial Fibrillation: update with NOAC Treatment and the impact of Reversal (Dr. Allison Kirsop)
Transition of ADHD Patients from Childhood into Adulthood (Dr Allison Kirsop)
An Introduction to the Internal Capsule in Schizophrenia (Dr. Matthew Williams)
About Oruen – The CNS Journal
The journal is owned and published bi-annually by Oruen Limited; it is a peer-reviewed, open access publication, and has received CME accreditation from the European Accreditation Committee in CNS (EACIC) with a 100% focus on original CNS research topics, and the latest advances, diagnoses, and treatment of CNS disorders. Oruen – The CNS Journal is distributed in print and electronically to thousands of physicians, researchers, academics, nurses, and related healthcare professionals with an interest in CNS disorders. Both subscription and access are free and there are no contributory author fees for publication. Papers submitted for publication are accepted based on their originality, likely impact on and relevance to clinical practice, data quality, and overall potential interest to the journal’s readership.

Dec 14, 2018
First published on ScienceDaily.com
Aggressive treatment of hypertension in stroke patients could do more harm than good in the long term, according to a new study from researchers at the University of Georgia.
Sixty percent of stroke patients admitted to U.S. emergency rooms have elevated blood pressure, and many studies say that having high blood pressure at the time of stroke can lead to higher rates of death and major disability.
But lowering blood pressure too much with medications may actually be working against the body’s protective response to maintain blood flow into the affected brain tissues.
“This presents a clinical dilemma,” said study author Changwei Li, an assistant professor of epidemiology and biostatistics at UGA’s College of Public Health.
It may be better to keep blood pressure a little higher than normal, closer to 140/90 mmHg rather than a “good” blood pressure of 120/80 mmHg, but that leaves the question of best practices a little open-ended.
“Currently, hypertension treatment for acute stroke patients is based on physicians’ clinical experience and judgement,” said Li. “There is no guideline on how low the blood pressure should be maintained.”
The key is to find the right balance between maintaining blood flow to the brain and reducing negative short- and long-term effects.
To help identify this optimal blood pressure, Li and his co-authors looked at the relationship between blood pressure during stroke and both short- and long-term health outcomes for over 4,000 Chinese stroke patients participating in the China Antihypertensive Trial in Acute Ischemic Stroke study. One group of stroke patients received extensive treatment for high blood pressure while a control group received no treatment at the time of their stroke.
Li and his collaborators tracked blood pressure changes over time in both the treatment and control groups during the first week of hospital admission and compared patient health at one week, three months, one year and two years following the stroke across patients of different blood pressure trajectories.
To access the full article, please click here.
Story Source:University of Georgia. “Optimal blood pressure treatment for stroke patients.” ScienceDaily. ScienceDaily, 10 December 2018. <www.sciencedaily.com/releases/2018/12/181210142059.htm>.

Dec 8, 2018
Jon Barrick, SAFE President, presented Stroke ACtion Plan for Europe 2018-2030 at the 13th UK Stroke Forum Conference (#UKSF18). The #UKSF18 took place at The International Centre, Telford,UK, from 4 – 6 December 2018.
“There was a great need for a document such as the Stroke Action Plan for Europe. Many European countries do not have a national stroke plan or strategy and many of them only have partial coverage of the stroke care pathway in their plans” said Barrick.
This 3 day multidisciplinary conference brought together over 110 expert speakers and researchers, all committed to improving stroke care.
About UK Stroke Forum
The UK Stroke Forum is a coalition of over 30 organisations all committed to improving stroke care in the UK. The coalition is underwritten by the Stroke Association UK.
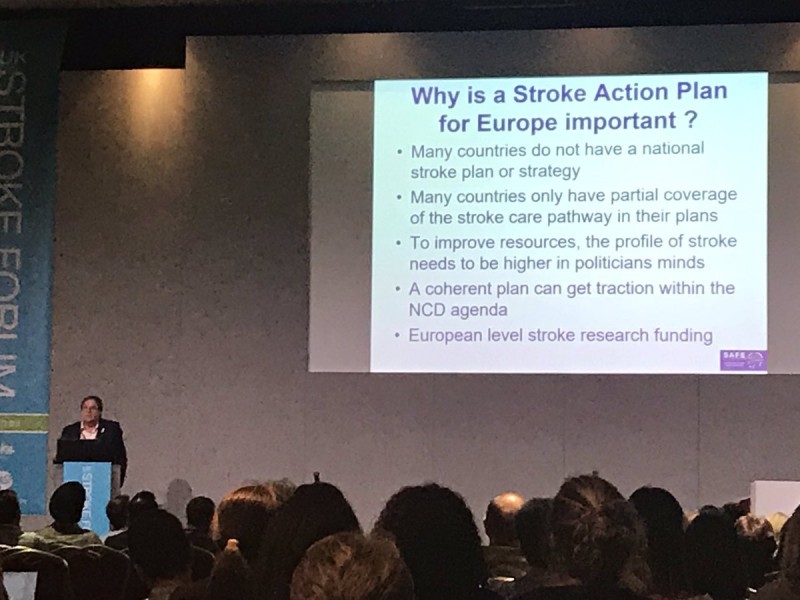
Photo by Sarah Belson



