
Apr 12, 2019
Author: Aidan Judd
In 2016 and 2017, broadcaster Mark Goodier suffered two strokes. He found when he got home from hospital, there were not that many resources to use as part of your recovery. And once you are away from constant medical supervision, it can be a lonely time as family and friends get back to their daily lives.
 Mark started the Stroke Stories podcast to seek out and hear from stroke survivors.
Mark started the Stroke Stories podcast to seek out and hear from stroke survivors.
In every episode, we hear a different stroke survivor – we hear about their condition, what inspires them, and the lessons they learned on the road to recovery.
Every stroke is different, and we reflect that in the people that we talk to for the podcast. Since November 2018, when the first episode was released, we’ve spoken to people from all different ages, backgrounds, and nationalities:
Nick and Jo Cann
Nick had a stroke when he was 50. After the stroke he found that there was a lack of support in his area for him and other stroke survivors. Despite suffering from aphasia, Nick speaks at events across the UK to raise awareness of stroke, and has also set up a support cafe meet up.
Connor and Sarah Lynnes
As a result of an injury he had whilst playing rugby, Connor had a massive stroke at just 14 years old. Connor has now set up his own foundation, to help other young survivors of stroke and brain injuries.
Clodagh Dunlop
A front-line police officer, Clodagh Dunlop was only 35 when she suffered her stroke. As a result, she experienced locked-in syndrome, which meant she was unable to move or speak. However, after 7 months of intense physiotherapy, she walked out of hospital, and is back working full time in the police force.
Antonio Iannella
Antonio suffered a stroke at the age of 38 whilst in holiday with his family in Vietnam. Since then, he has recovered well, and pursued a lifelong dream of opening and running a music recording studio in his home.
We want to spread the message as far as possible. If you are a stroke survivor and would like to feature in a future episode, then please contact SAFE, or DM us via our Twitter account – twitter.com/strokestories
Updated with new episode released every week, Stroke Stories seeks to inspire and reassure with real life stories from stroke survivors and their families.
There are currently over 20 episodes available through iTunes (https://itunes.apple.com/gb/podcast/stroke-stories/id1442493312?mt=2) and on ACast (https://play.acast.com/s/strokestories)
For the latest updates, follow Stroke Stories on Twitter – www.twitter.com/strokestories and Instagram www.instagram.com/strokestories
Apr 12, 2019
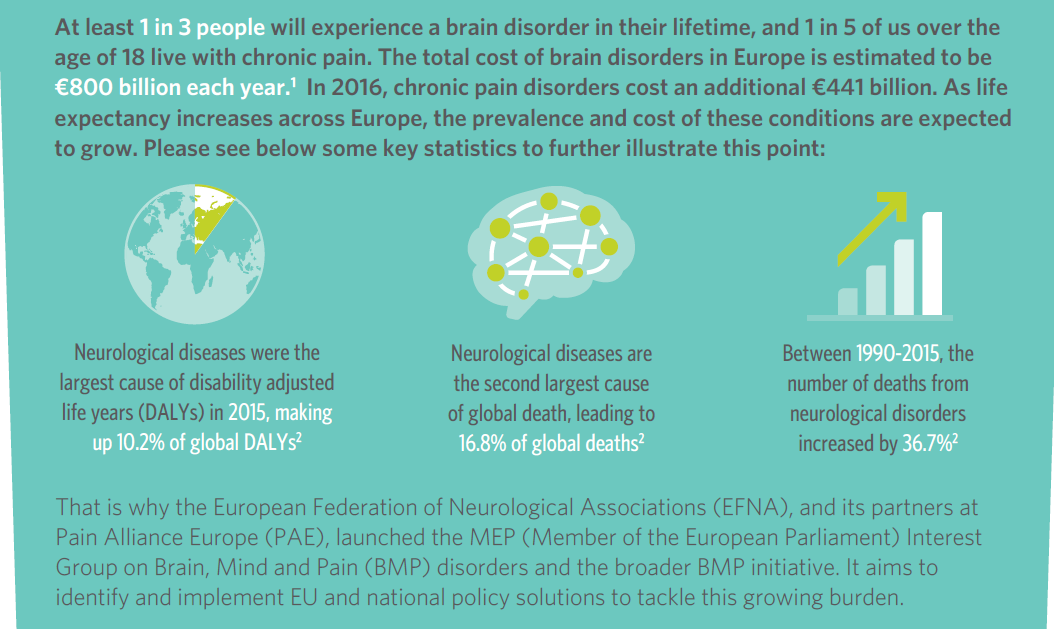
The Brain, Mind and Pain (BMP) initiative has today launched its Book of Evidence for the 2019-2024 EU mandate.
This Book of Evidence (BoE) sets a strategic vision on policy action to deliver better care for people with neurological and chronic pain disorders in the EU.
It will be used as the core policy document of the MEP Interest Group on Brain, Mind & Pain – which will continue after the upcoming EU elections for the next 5 year mandate.
The Interest Group is coordinated by European Federation of Neurological Associations (EFNA) and Pain Alliance Europe (PAE).
 The BoE outlines clear focus areas and proposes recommendations for policy actions, which, if implemented, would significantly improve quality of life for people with neurological and chronic pain disorders, as well as their families and carers.
The BoE outlines clear focus areas and proposes recommendations for policy actions, which, if implemented, would significantly improve quality of life for people with neurological and chronic pain disorders, as well as their families and carers.
The development of the document was led by EFNA and PAE and involved a wide range of key EU and national stakeholders from the patient, policy, industry and scientific communities.
This collaborative development process is reflected in wide ranging endorsements and support from organisations such as the European Commission, European Brain Council, European Patients’ Forum, European Academy of Neurology, European Pain Federation and European Alliance for Patient Access.
Key areas for action
The BoE outlines the thematic areas of focus for the MEP Interest Group on Brain, Mind and Pain for the 2019-2024 mandate. These are:
» Eradicate stigma, isolation and discrimination: A lack of public awareness of BMP disorders feeds their stigma and the associated isolation and discrimination suffered by BMP patients, carers, and their families.
» Ensure equitable access to treatment, services, and support: Access to treatment, services, and support is a topic of concern for patients in Europe due to high failure rates, delays in market access, relatively expensive treatments, and inequality in access across, but also within, EU Member States
» Promote patient empowerment for increased involvement and engagement: Patient empowerment is a means for more effective BMP patient engagement and meaningful involvement in the research, medical and policy conversations which affect them
These areas have been chosen in order to support the MEP Interest Group in leveraging current policy opportunities on the agenda whilst ensuring continuity with the past activities and successes of the BMP initiative.
Driving policy change
The 2019-2024 mandate brings with it an active policy environment at EU level, with numerous opportunities for advocacy on behalf of people with brain, mind and pain disorders.
Ensuring that the Interest Group is capable of impacting policy discussions throughout the 2019-2024 mandate will be key in making progress in the three key thematic areas identified.
Additionally, with the global priority turning more and more towards NCDs, we need to ensure that brain, mind and pain disorders are part of global health policy agenda.
To this end, each chapter of the BoE contains a section on the policy opportunities and subsequent actions that can be leveraged to further progress in each thematic area and at EU and global level.
Looking ahead
It is now the responsibility of the Interest Group and the wider BMP initiative to leverage the policy opportunities and pursue the policy actions identified in this text throughout the 2019-2024 mandate.
EFNA President, Joke Jaarsma says: ‘Progress is contingent on coordinated policy advocacy at EU and global level, taken forward by the BMP initiative as a whole and its partners.
‘Using the BoE as a springboard for action, let’s drive policy change and make a real difference to the daily lives of people living with BMP disorders across Europe!’ she continued.
For any further information on the BoE or the activities of the BMP initiative – including its MEP Interest Group – please do not hesitate to contact EFNA at: advocacy@efna.net
For more contact:
Tadeusz Hawrot
EFNA Senior Advocacy Coordinator
advocacy@efna.eu
Elizabeth Cunningham
EFNA Communications Manager
communications@efna.eu

Apr 9, 2019
This year’s main theme for SAFE’s campaigning work is Life After Stroke, the issues around it and how the stroke survivors and their families are coping with it. The campaign will cover this year’s European Stroke Awareness Day in May and will culminate on October 29, for the World Stroke Day, when SAFE will present the Economic Impact of Stroke in Europe Report.
Stroke is responsible for 9% of all deaths each year in the EU and it is also the largest cause of adult disability. Total costs for stroke were estimated at €64 billion across Europe in 2010 and yet it is hugely under-funded in comparison to other chronic conditions. The most important risk factors for stroke are age, high blood pressure, obesity and diabetes, all of which are rising in a larger and increasingly elderly population living unhealthy lifestyles. Recent modest improvements in acute care mean that more people are surviving stroke, but with impairment, with the consequence that we have a major health economic and social burden catastrophe waiting to happen. This will severely impact all EU countries but especially those where inequalities in stroke healthcare are already known.
In 2017, SAFE has commissioned a research project on the economic impact of stroke in Europe. A health economics team from the University of Oxford is now finalising the report, which will be launched by SAFE in October 2019, for the World Stroke Day.
In anticipation of the final results, SAFE would like to remind the public that the absolute number of people living with disability from stroke has been increasing over the past three decades, and this is projected to increase. LMICs (low and middle income countries) have been disproportionately affected by stroke, and disability-adjusted life years (DALYs) from stroke have been generally increasing in LMICs.(1)
For this reason, SAFE is opening a conversation stream with leaders of our member organisations from 30 European countries. Each week, our readers will have an opportunity to read about one burning life after stroke issue in different countries. The series of interviews will shed light on specific country by country needs of stroke survivors and their families.
The slogan of this year’s campaign is: A life saved must also be lived, by Grethe Lunde from Norway, a Stroke Survivor and SAFE Board member.
(1) Feigin VL, Norrving B, Mensah GA. Global Burden of Stroke. Circ Res. (2017) 120:439–48. 10.1161/CIRCRESAHA.116.308413

Apr 8, 2019
First published on ScienceDaily.com
The full financial cost of a heart attack or stroke is twice as much as the medical costs when lost work time for patients and caregivers is included.
That’s the finding of research published today, World Health Day, in the European Journal of Preventive Cardiology, a journal of the European Society of Cardiology (ESC).1 The study concludes that victims of heart attack and stroke who return to work are 25% less productive in their first year back.
In the year after the event, heart patients lost 59 workdays and caregivers lost 11 workdays, for an average cost of €13,953, and ranging from €6,641 to €23,160 depending on the country. After stroke, 56 workdays were lost by patients and 12 by caregivers, for an average €13,773, ranging from €10,469 to €20,215.
Study author Professor Kornelia Kotseva, of Imperial College London, UK, said: “Patients in our study returned to work, meaning their events were relatively mild. Some still had to change jobs or careers, or work less, and caregivers lost around 5% of work time. Not included in our study are those with more severe events who quit work altogether and presumably need even more help from family and friends.”
The study enrolled 394 patients from seven European countries — 196 with acute coronary syndrome (86% heart attack, 14% unstable chest pain) and 198 with stroke — who returned to work 3 to 12 months after the event. Patients completed a questionnaire2,3 during a visit to a cardiologist, neurologist, or stroke physician. Hours lost were valued according to country labour costs in 2018. The average age of patients was 53 years.
According to published estimates for Europe, the direct medical costs of acute coronary syndrome are €1,547 to €18,642, and €5,575 to €31,274 for stroke.4 “This is the metric commonly used to estimate the costs of medical conditions while indirect costs from productivity loss are often not taken into account by clinicians, payers or policymakers,” said Professor Kotseva. “Taken together, the actual burden on society is more than twice the amount previously reported.”
You can read the full article here.

Apr 7, 2019
First published on ScienceDaily.com
Newly developed treatment strategies can minimize the size of a patient’s stroke and, in many cases, change what would have been a life-altering cerebrovascular event into a minor one with the prospect of excellent recovery. But these therapies are time sensitive — delays in seeking care can put them out of reach. Each year in the U.S., 795,000 patients will have a stroke and approximately 70 percent of them will arrive at the hospital more than six hours after the onset of symptoms. Investigators from Brigham and Women’s Hospital examined how social networks may influence delays in arrival times for patients experiencing the symptoms of a stroke. Paradoxically, they found that patients with closer-knit social networks, including family members and spouses, were more likely to delay seeking hospital care whereas those with a more dispersed network of acquaintances were more likely to seek care faster. The team’s analysis is published in Nature Communications.
“Closed networks are like echo chambers in which there is a tendency for everyone to agree to watch and wait,” said corresponding author Amar Dhand, MD, DPhil, of the Department of Neurology at the Brigham. “A major problem in stroke care is patients’ delayed arrival to the hospital, and we show that this problem is related to the influence of patients’ social networks.”
Dhand and colleagues surveyed 175 patients within five days of suffering from a stroke. They collected information from each participant about personal social networks, creating network maps. The team focused on patients with milder symptoms because this population is at higher risk for delay and were able to engage in the survey during hospitalization.
You can read the full article here.


