
Apr 16, 2019
This article first appeared on the PREvention of Stroke in Intracerebral haemorrhaGE survivors with Atrial Fibrillation (PRESTIGE-AF) website
The PRESTIGE-AF team are going to Milan in May to participate in one of Europe’s leading forums for stroke research, the European Stroke Organisation Conference (ESOC).
The European Stroke Organisation Conference is a premier European forum for stroke research and rapidly becoming the global platform for the release of major trial data. Last year the conference welcomed over 4,500 participants from around the world with 1800 abstracts submitted, and over 1300 e-posters on display. With one participant suggesting “it is the stroke conference in Europe I think at the moment (participant from ESOC 2019 promotional video), the 2019 conference will provide a unique opportunity for the PRESTIGE-AF team to network with fellow clinicians and scientists.
The PRESTIGE-AF team will present, discuss and trade expertise in the most rapidly evolving area of stroke management and care. We have quite a few from the PRESTIGE-AF team presenting at the conference including the project’s coordinators from Imperial College London, Roland Veltkamp, Stephanie Debette from Universite de Bordeaux, and Joan Montaner from Vall d’Hebron Research Institute (VHIR). Roland will convene the session on Intracerebral Haemorrhage and do a short presentation looking at the causes of recurrent ischemic stroke after embolic stroke of an undetermined source. The team will take full advantage of the conference with holding their own Investigator Meeting and Steering Committee breakfast.
ESO president Bart van der Worp, notes that “ESOC 2019 will be even greater…with major trial results to be presented” (ESOC Youtube Video), so we are looking forward to the team’s review of the conference including presentations of major clinical trials.
Go to the website for more information about the 2019 European Stroke Organisation Conference.

Apr 12, 2019
As announced earlier, SAFE will open conversation with our member organisations’ leaders, in the attempt of shedding light on life after stroke issues across Europe.
This week we are talking with Dr Maja Bozinovska Smiceska, President of Association for a fight against stroke “Stroke” in North Macedonia.
SAFE: What is one issue related to the life after stroke in your country that you think needs special attention?
 MBS: Every stroke is different, and so is the recovery that follows. Patients suffer not just physical problems like weakness and impaired gait, but also difficulties with language, memory, cognition and emotional problems. Patients everyday life changes and become full of obstacles and frustration.
MBS: Every stroke is different, and so is the recovery that follows. Patients suffer not just physical problems like weakness and impaired gait, but also difficulties with language, memory, cognition and emotional problems. Patients everyday life changes and become full of obstacles and frustration.
One aspect regarding rehabilitation in their recovery is intensive work with multidisciplinary team. So, the first problem in our country is deficiency of such team in most of our cities or inequality in specialized stroke recovery. All stroke survivors have approach to physical therapy, part of them of them have language therapy at disposal, but just a small percentage have luck to be rehabilitated by a multidisciplinary team.
Second very important problem is that there is no national strategy, a specific path, that will simplify the struggle of patient and family. Considering not just rehabilitation but also their adaptation to situation and inclusion in society, helping them to be productive as possible or providing to others specific help according to their needs like financial help or accommodation.
SAFE: What would be the solution, i.e. what is your organisation’s position regarding this issue?
MBS: As the only organisation that deals with stroke patients in our country, we are continuously increasing public awareness and educating public using different media, where and how to find help and to whom to address their specific problems. Also our network is offering annually reviewed data. We organise lectures for specific groups considering certain post stroke problems. Our organisation in 2017 formed a special team consisting of Stroke neurologists, nurses stroke survivors and caregivers that created a document in which we included recommendations for life after stroke. Members of our team already had two meeting in Ministry of health of Northern Macedonia, and this document was given to the counselor of the minister. What we consider important is forming a team in Ministry of health that deals with the issues of stroke, generally they should create and implement national strategy.
Our next goal is to organise peer to peer meetings and that way to improve self-management in stroke survivors and caregivers.
SAFE: Please tell us more about your organisation.
MBS: Our organisation is formed 2014. Our idea was to improve stroke care in our country that was very poor and unequal in different regions. Main goals of our organisation are raising the consciousness of the public and education; join care for improving the health condition of the patients with a stroke; informing about the new scientific and practical achievements in the treatment of the patients with a stroke; providing professional help in the field of action; encouraging and strengthening the cooperation with domestic and foreign organisations and institutions which have same or similar goals. We started with activities for stroke prevention and post stroke consultations for patients and caregivers that included not just spreading information trough media but also field work of teams consisting different specialists, doctors, nurses, clinical psychologists and physiotherapists in different cities. These activities are still going on, and we have upgraded our work. Our organisation is now member of SAFE and WSO.

Apr 12, 2019
Author: Aidan Judd
In 2016 and 2017, broadcaster Mark Goodier suffered two strokes. He found when he got home from hospital, there were not that many resources to use as part of your recovery. And once you are away from constant medical supervision, it can be a lonely time as family and friends get back to their daily lives.
 Mark started the Stroke Stories podcast to seek out and hear from stroke survivors.
Mark started the Stroke Stories podcast to seek out and hear from stroke survivors.
In every episode, we hear a different stroke survivor – we hear about their condition, what inspires them, and the lessons they learned on the road to recovery.
Every stroke is different, and we reflect that in the people that we talk to for the podcast. Since November 2018, when the first episode was released, we’ve spoken to people from all different ages, backgrounds, and nationalities:
Nick and Jo Cann
Nick had a stroke when he was 50. After the stroke he found that there was a lack of support in his area for him and other stroke survivors. Despite suffering from aphasia, Nick speaks at events across the UK to raise awareness of stroke, and has also set up a support cafe meet up.
Connor and Sarah Lynnes
As a result of an injury he had whilst playing rugby, Connor had a massive stroke at just 14 years old. Connor has now set up his own foundation, to help other young survivors of stroke and brain injuries.
Clodagh Dunlop
A front-line police officer, Clodagh Dunlop was only 35 when she suffered her stroke. As a result, she experienced locked-in syndrome, which meant she was unable to move or speak. However, after 7 months of intense physiotherapy, she walked out of hospital, and is back working full time in the police force.
Antonio Iannella
Antonio suffered a stroke at the age of 38 whilst in holiday with his family in Vietnam. Since then, he has recovered well, and pursued a lifelong dream of opening and running a music recording studio in his home.
We want to spread the message as far as possible. If you are a stroke survivor and would like to feature in a future episode, then please contact SAFE, or DM us via our Twitter account – twitter.com/strokestories
Updated with new episode released every week, Stroke Stories seeks to inspire and reassure with real life stories from stroke survivors and their families.
There are currently over 20 episodes available through iTunes (https://itunes.apple.com/gb/podcast/stroke-stories/id1442493312?mt=2) and on ACast (https://play.acast.com/s/strokestories)
For the latest updates, follow Stroke Stories on Twitter – www.twitter.com/strokestories and Instagram www.instagram.com/strokestories
Apr 12, 2019
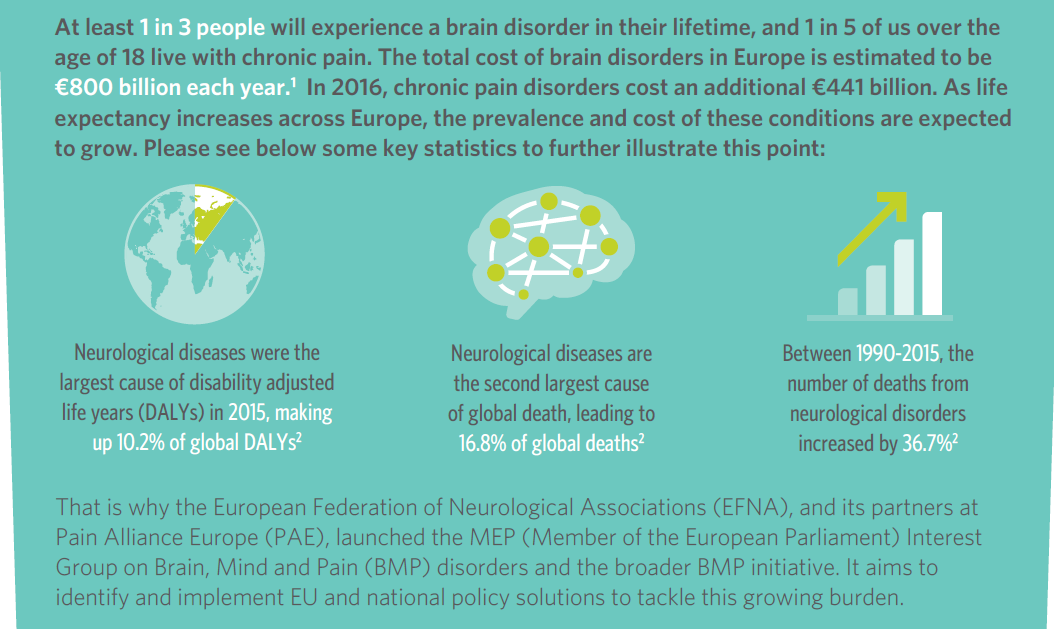
The Brain, Mind and Pain (BMP) initiative has today launched its Book of Evidence for the 2019-2024 EU mandate.
This Book of Evidence (BoE) sets a strategic vision on policy action to deliver better care for people with neurological and chronic pain disorders in the EU.
It will be used as the core policy document of the MEP Interest Group on Brain, Mind & Pain – which will continue after the upcoming EU elections for the next 5 year mandate.
The Interest Group is coordinated by European Federation of Neurological Associations (EFNA) and Pain Alliance Europe (PAE).
 The BoE outlines clear focus areas and proposes recommendations for policy actions, which, if implemented, would significantly improve quality of life for people with neurological and chronic pain disorders, as well as their families and carers.
The BoE outlines clear focus areas and proposes recommendations for policy actions, which, if implemented, would significantly improve quality of life for people with neurological and chronic pain disorders, as well as their families and carers.
The development of the document was led by EFNA and PAE and involved a wide range of key EU and national stakeholders from the patient, policy, industry and scientific communities.
This collaborative development process is reflected in wide ranging endorsements and support from organisations such as the European Commission, European Brain Council, European Patients’ Forum, European Academy of Neurology, European Pain Federation and European Alliance for Patient Access.
Key areas for action
The BoE outlines the thematic areas of focus for the MEP Interest Group on Brain, Mind and Pain for the 2019-2024 mandate. These are:
» Eradicate stigma, isolation and discrimination: A lack of public awareness of BMP disorders feeds their stigma and the associated isolation and discrimination suffered by BMP patients, carers, and their families.
» Ensure equitable access to treatment, services, and support: Access to treatment, services, and support is a topic of concern for patients in Europe due to high failure rates, delays in market access, relatively expensive treatments, and inequality in access across, but also within, EU Member States
» Promote patient empowerment for increased involvement and engagement: Patient empowerment is a means for more effective BMP patient engagement and meaningful involvement in the research, medical and policy conversations which affect them
These areas have been chosen in order to support the MEP Interest Group in leveraging current policy opportunities on the agenda whilst ensuring continuity with the past activities and successes of the BMP initiative.
Driving policy change
The 2019-2024 mandate brings with it an active policy environment at EU level, with numerous opportunities for advocacy on behalf of people with brain, mind and pain disorders.
Ensuring that the Interest Group is capable of impacting policy discussions throughout the 2019-2024 mandate will be key in making progress in the three key thematic areas identified.
Additionally, with the global priority turning more and more towards NCDs, we need to ensure that brain, mind and pain disorders are part of global health policy agenda.
To this end, each chapter of the BoE contains a section on the policy opportunities and subsequent actions that can be leveraged to further progress in each thematic area and at EU and global level.
Looking ahead
It is now the responsibility of the Interest Group and the wider BMP initiative to leverage the policy opportunities and pursue the policy actions identified in this text throughout the 2019-2024 mandate.
EFNA President, Joke Jaarsma says: ‘Progress is contingent on coordinated policy advocacy at EU and global level, taken forward by the BMP initiative as a whole and its partners.
‘Using the BoE as a springboard for action, let’s drive policy change and make a real difference to the daily lives of people living with BMP disorders across Europe!’ she continued.
For any further information on the BoE or the activities of the BMP initiative – including its MEP Interest Group – please do not hesitate to contact EFNA at: advocacy@efna.net
For more contact:
Tadeusz Hawrot
EFNA Senior Advocacy Coordinator
advocacy@efna.eu
Elizabeth Cunningham
EFNA Communications Manager
communications@efna.eu

Apr 9, 2019
This year’s main theme for SAFE’s campaigning work is Life After Stroke, the issues around it and how the stroke survivors and their families are coping with it. The campaign will cover this year’s European Stroke Awareness Day in May and will culminate on October 29, for the World Stroke Day, when SAFE will present the Economic Impact of Stroke in Europe Report.
Stroke is responsible for 9% of all deaths each year in the EU and it is also the largest cause of adult disability. Total costs for stroke were estimated at €64 billion across Europe in 2010 and yet it is hugely under-funded in comparison to other chronic conditions. The most important risk factors for stroke are age, high blood pressure, obesity and diabetes, all of which are rising in a larger and increasingly elderly population living unhealthy lifestyles. Recent modest improvements in acute care mean that more people are surviving stroke, but with impairment, with the consequence that we have a major health economic and social burden catastrophe waiting to happen. This will severely impact all EU countries but especially those where inequalities in stroke healthcare are already known.
In 2017, SAFE has commissioned a research project on the economic impact of stroke in Europe. A health economics team from the University of Oxford is now finalising the report, which will be launched by SAFE in October 2019, for the World Stroke Day.
In anticipation of the final results, SAFE would like to remind the public that the absolute number of people living with disability from stroke has been increasing over the past three decades, and this is projected to increase. LMICs (low and middle income countries) have been disproportionately affected by stroke, and disability-adjusted life years (DALYs) from stroke have been generally increasing in LMICs.(1)
For this reason, SAFE is opening a conversation stream with leaders of our member organisations from 30 European countries. Each week, our readers will have an opportunity to read about one burning life after stroke issue in different countries. The series of interviews will shed light on specific country by country needs of stroke survivors and their families.
The slogan of this year’s campaign is: A life saved must also be lived, by Grethe Lunde from Norway, a Stroke Survivor and SAFE Board member.
(1) Feigin VL, Norrving B, Mensah GA. Global Burden of Stroke. Circ Res. (2017) 120:439–48. 10.1161/CIRCRESAHA.116.308413
Apr 4, 2019
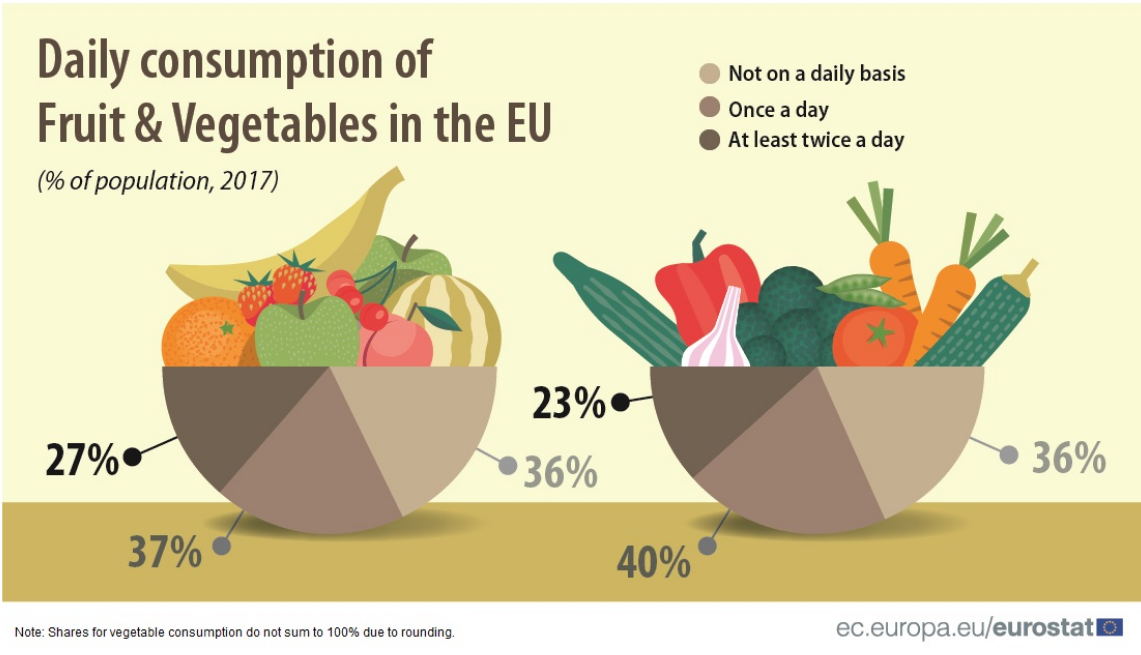
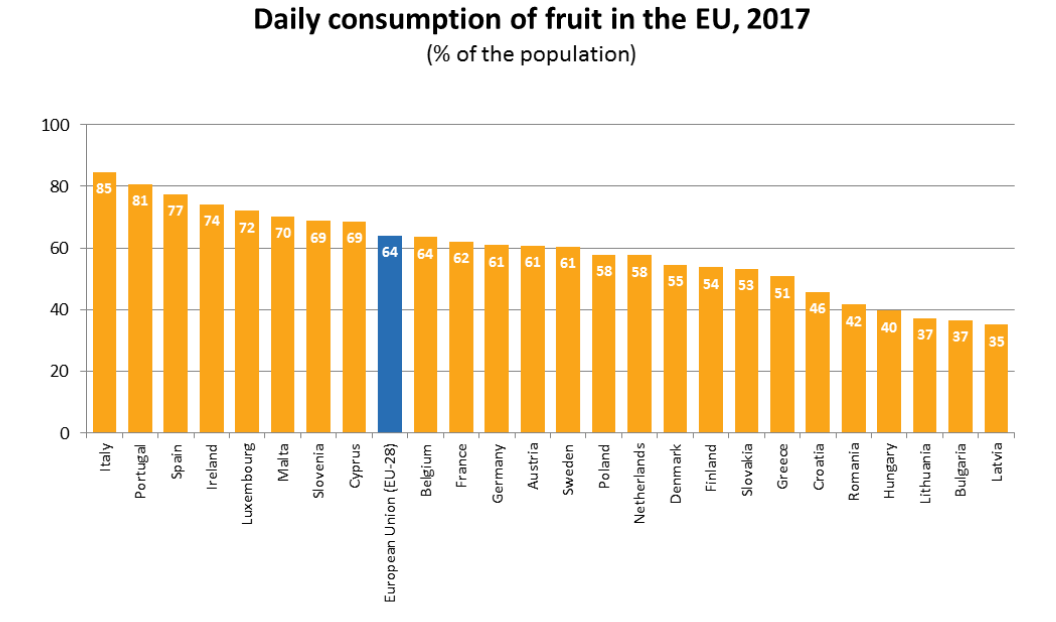
In 2017, around 1 in 4 people (27 %) ate fruit at least twice a day, according to a survey of the European Union (EU) population. A further 37 % of the EU population ate fruit once a day and the remaining 36 % ate fruit either less frequently or not at all during a typical week. Compared with fruit consumption, a slightly smaller proportion (23 %) of the EU population ate vegetables at least twice a day, and a slightly higher proportion (40 %) ate vegetables once a day. Among the EU Member States, daily intake of fruit was most prevalent in Italy (85 % of the population) and in Portugal (81 %).
The source data are here.
In contrast, in three Member States less than 40 % of the population ate fruit on a daily basis: Latvia (35 %), Bulgaria and Lithuania (both 37 %). When it comes to vegetable consumption in the Member States, Ireland and Belgium had the highest proportion of the population who ate vegetables at least once a day (both 84 %). While in most Member States between 50 % and 80 % of the population reported that they ate vegetables daily, there were five Member States where the proportion was below 50 %: Hungary (30 %), Romania (41 %), Latvia (44 %), Lithuania and Bulgaria (both 45 %).
For more information from this report, please click here.


