
May 7, 2020
Press release by Portugal AVC
The Portuguese association of stroke survivors – PT.AVC – cautions about the consequences of the current health crisis on stroke care. Stroke is the first cause of death and disability in Portugal.
In a survey performed between 20th and 27th April and to which 868 Portuguese stroke survivors responded, 91% of all patients indicated for rehabilitation treatment reported that they had to stop or were unable to start this intervention. This is particularly worrisome as there is compelling evidence that delays in rehabilitation are associated with a greater likelihood of long-term disability, thus undermining social integration and leading to worse quality of life.
Moreover, only 15% of the respondents had their follow-up medical visits since the beginning of the pandemic and, amongst those stroke survivors still under medical attention, about half had also their scheduled medical examinations cancelled or postponed.
Overall, about one third of the respondents reported felling that their health was worse or much worse than before the outbreak and, among those who had a stroke within the previous year, this proportion raised to 50%.
Most of the participants confirmed several complaints, such as feeling anxious, experiencing worsening of motor and/or speech difficulties and increased concerns with regards to recovery and risk of stroke recurrence.
Importantly, 38% stated that the current situation is having a negative effect on their financial situation, which we know is often already impaired.
PT.AVC thus emphasises that, during the reopening phase that is now starting, investment in expansion, adaptation and reorganization of rehabilitation services is imperative, with maintained quality. The Portuguese association of stroke survivors also highlights that all efforts have to be done to maintain rehabilitation care, which should be considered in future decisions as an essential health service for priority cases, and warns stakeholders that it is crucial to avoid the serious consequences that inappropriate stroke care has in the prognosis of affected patients, which can potentially lead to even more devastating consequences that those related with the coronavirus infection itself.
Apr 15, 2020
 The EU funded TENSION project examines the effects of mechanical clot retrieval in a large group of patients in whom the benefit of thrombectomy is uncertain. TENSION studies if it is safe and effective to do thrombectomy in patients with so-called ‘extended lesions’, that is, larger areas of damaged brain when compared to the previous studies. Patients are also able to enroll in the trial up to 12 hours after their symptoms first showed. This extends the treatment to a larger group of patients: including, for instance, more of those who have a stroke during the night-time and are more likely to be delayed in getting to hospital. We interviewed Dr. Claus Simonsen from the Department Of Neurology, Aarhus University Hospital, Denmark.
The EU funded TENSION project examines the effects of mechanical clot retrieval in a large group of patients in whom the benefit of thrombectomy is uncertain. TENSION studies if it is safe and effective to do thrombectomy in patients with so-called ‘extended lesions’, that is, larger areas of damaged brain when compared to the previous studies. Patients are also able to enroll in the trial up to 12 hours after their symptoms first showed. This extends the treatment to a larger group of patients: including, for instance, more of those who have a stroke during the night-time and are more likely to be delayed in getting to hospital. We interviewed Dr. Claus Simonsen from the Department Of Neurology, Aarhus University Hospital, Denmark.
SAFE: If you were to explain the project’s aim to a person without any medical background, what would you say?
CS: Stroke treatment is advancing. The majorities of stroke are caused by an occlusion of an artery. Removal of the clot/occlusion means that the patient will do much better. If the clot is big, we can remove it with a catheter. This is a great idea, if the damage to the brain is small. If there is more advanced damage, we don’t know, if the patient benefit from removal of the clot. The project will try to prove, that these patients also benefit. Then we can treat and help more patients.
SAFE: What types of partner do you need to carry out a project like this?
CS: To be a partner in the project, you need to have a thrombectomy centre. And you probably need a relatively big catchment area. There are not many patients with advanced damage who at the same time fulfil all inclusion criteria. Your staff should have some experienced in trials and inclusion in trials. A research nurse would be very good.
SAFE: Can you briefly describe your role in the project?
CS: I am the PI (principal investigator) in Denmark. I am in contact with the trial managers and with the monitors in Denmark. I try to include more Danish centres in the trial. And I try to increase inclusion at my own centre by reminding colleagues about the trial.
SAFE: What (if any) are the difficulties with carrying out the work?
CS: Difficulties: To keep everyone informed about the project. To randomize patients that we (sometimes) would have treated. To get consent from relatives in a critical situation. (We randomize without consent in Denmark, but we need consent from the relatives for the patients to stay in the project.)
SAFE: What personally attracted you to be in this project?
CS: Acute stroke treatment is my big research interest. This topic (treatment of patients with big strokes and advanced damage) is one of the most interesting areas in stroke treatment.
SAFE: When this project ends, what do you expect to change, i.e. how it will reflect on stroke treatment?
CS: I think the project will be positive. (Otherwise, I would probably not contribute.) So I think we can treat more patients after the project is over. Or we will be more informed when we are making treatment decisions for this patient group.
The TENSION trial has received funding from the European Union’s Horizon 2020 research and innovation programme under grant agreement No. 754640.
Image credit: Frederik Denorme

Apr 9, 2020
The Exercise Guide for stroke survivors in the Netherlands was developed some years ago, in collaboration of the medical experts from the University of Utrecht, other allied stroke professionals and Dutch stroke survivors. This booklet is usually being given to patients during their stay in the hospital or while in rehabilitation. The guide itself will be free (temporarily) for everybody. Small SSO’s can get the rights to translate in their own language for free, while the larger SSO’s will be asked to pay a small fee.
“In these crazy Corona times most Dutch stroke survivors do not get physical therapy anymore, as everything is on hold or locked down. It is important for everybody, but especially for them, to keep exercising and we are convinced this guide is a great solution for that” says Monique Lindhout, the Director of Hersenletsel.nl, adding that “Sharing with others in need and helping them in times of crisis not only makes us feel good, it also brings a real-life change for the stroke patients affected.”
The Exercise Guide is a practical tool for patients to start exercising independently from day one after a stroke. The exercises are all easy to perform either lying in bed or sitting in a chair. The exercises are divided into three levels of complexity each indicated by a different colour, and, as much as possible, everyday activities are included in the given exercises.
The benefits in using this exercise guide
According to therapists, nurses and patients, the exercise guide is a powerful and low-cost tool to intensify rehabilitation treatment for patients after stroke without the need for extra personnel.

The front cover of the Exercise Guide
How to get your copy of the Exercise Guide e-book?
The e-Version of this guide will be only temporarily available for free. Hurry up and click here to follow instructions and download your own copy of the Exercise Guide.
Background
The exercise guide was developed in 2010 in the Netherlands by the University Medical Centre Utrecht and Rehabilitation Centre De Hoogstraat in collaboration with professionals of seven hospitals, rehabilitation centers and nursing homes and patients of the Dutch stroke patients association. In 2013, the exercise guide was translated into English. Currently the guide is being translated in Vietnamese and Thai. The guide is also available as an app (only in Dutch) for Apple and Android. The app is temporarily available for free.
Contact
For contact and suggestions about the Exercise Guide:
Monique Lindhout | moniquelindhout@hersenletsel.nl
Featured image by Niek Verlaan from Pixabay

Apr 8, 2020
Press Release by ESO | 8.4.2020 | ESO, Stroke Research
The European Stroke Organisation (ESO) cautions against the consequences of the Coronavirus-Crisis on stroke care.
Basel, 08 April 2020 – Each year, 1.5 million Europeans have a stroke. Two to three of every 10 patients die as a consequence of stroke, and about one third remain dependent on the help of others. The likelihood of a favourable outcome is critically dependent on patients presenting promptly after symptom onset and on hospitals providing immediate access to optimised stroke care. This includes treatments for vessel recanalisation, securing brain vascular malformations, specialised stroke unit care, secondary prevention, and rehabilitation.
In a survey among 426 stroke care providers from 55 countries, only one in five reported that stroke patients are currently receiving the usual acute and post-acute care at their hospital. The lack of optimal care is likely to lead to a greater risk of death and a smaller chance of a good recovery.
There is no reason to assume that the incidence of stroke declined since the onset of the COVID-19 crisis, but in many countries, fewer people with symptoms suggestive of stroke present to the hospital. This may be due to a range of factors, including fear to become infected with COVID-19 in the hospital or the assumption that doctors are too busy treating patients with COVID-19 to treat patients with stroke.
ESO supports the efforts to manage to COVID-19 pandemic and to treat patients with COVID-19, but emphasises that patients with stroke symptoms should still present to hospital as soon as possible and that efforts should be made to maintain the usual level of stroke care, including intravenous and endovascular reperfusion strategies, irrespective of the patient’s COVID-19 status, to avoid unnecessary ‘collateral damage’ through inadequate treatment of this often disabling or life-threatening condition.
Issued by the ESO Executive Committee.
Contact: esoinfo@eso-stroke.org
Image by Gerd Altmann from Pixabay
Apr 2, 2020
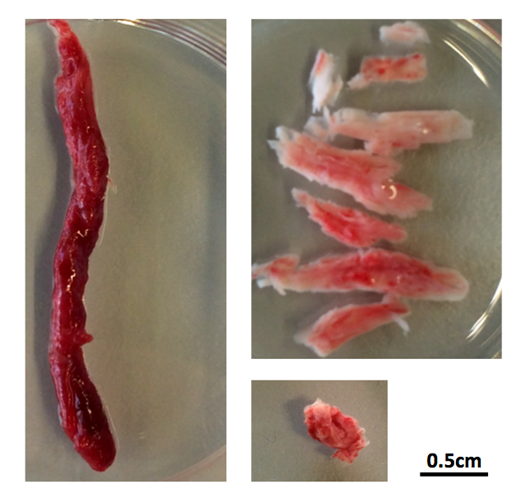
Damage to the small blood vessels in the brain (known as „Small Vessel Disease“) can lead to stroke and vascular dementia.
Despite causing these important conditions small vessel disease remains relatively poorly understood compared to other blood vessel diseases. With the better understanding of small vessel diseases, the study SVDs@target will develop novel therapeutic treatments and finally contribute to the prevention of stroke and dementia.
The project also includes 3 studies with stroke patients. They are:
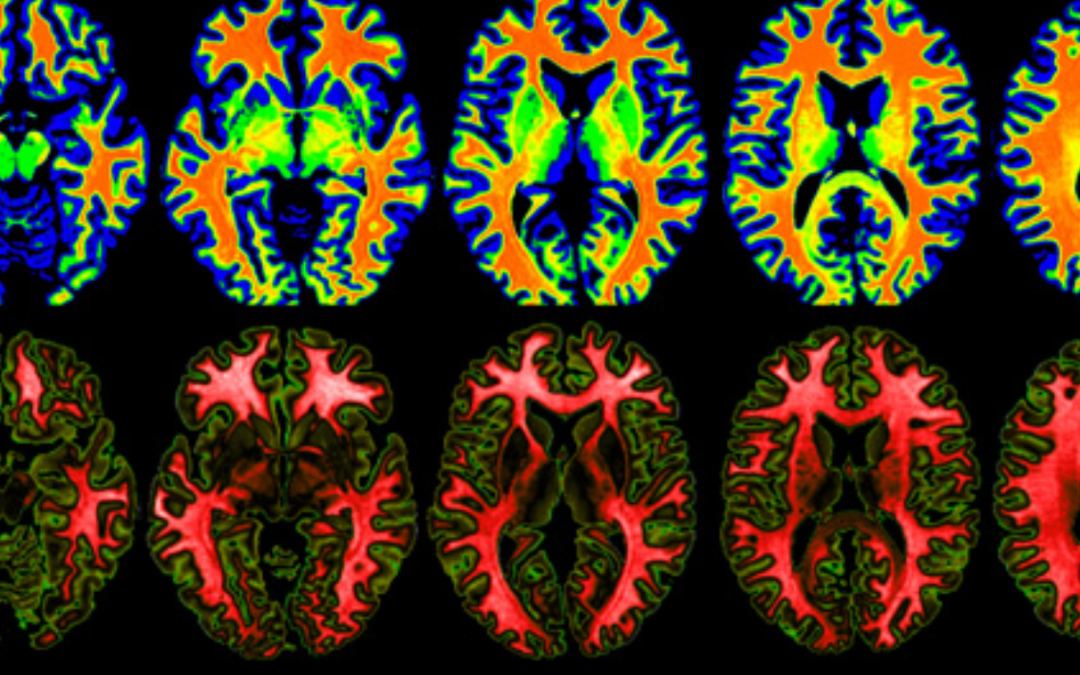
ZOOM@SVDs, a high-resolution imaging study to look at vascular function and brain damage
INVESTIGATE-SVDs, an imaging study to assess the blood/brain barrier and vascular function,
TREAT-SVDs, testing the effects of different blood pressure lowering agents on vascular function in patients with distinct SVDs
Michael Stringer_UEDIN
We spoke with Michael Stringer, Research Fellow in Magnetic Resonance Imaging and Image Analysis from the Centre for Clinical Brain Sciences, Edinburgh Imaging and the UK Dementia Research Institute at the University of Edinburgh.
Why does this trial (Zoom/INVESTIGATE or TREAT) on small vessel diseases matter?
Investigate-SVDs recruits small vessel disease (SVD) patients to have advanced magnetic resonance imaging scans. SVD remains poorly understood, this study has great potential to further knowledge & ultimately improve outcomes for patients.
What is it that you do in this project?
As a research fellow in medical physics at the University of Edinburgh I helped setup the magnetic resonance imaging protocol (guide to running the scans), liase with other sites and am heavily involved with analysis of the imaging data.
Why do you do it?
My research focuses on applying advanced imaging and mathematical methods to study disease. I enjoy applying these tools to study real world problems, and as a highly multidisciplinary area it provides a lot of variety – it is seldom dull.
SVDs@target has received funding from the European Union’s Horizon 2020 research and innovation programme under grant agreement No 666881.
Photo credit: A print screen from the official SVDs@Target website.

Apr 2, 2020
The European Federation of Neurological Associations (EFNA) are pleased to publish a position paper on ‘Advocating for access to neurology treatment, services and support’. The document is based on feedback from an EFNA workshop held in Warsaw in October 2019, attended by approximately 50 representatives of patient and health professional organisations, industry partners and other experts. The contents of this paper reflect the insightful and lively debates and the arising conclusions and recommendations.
These outputs have been captured to inform EFNA’s strategic plan for 2020-2025, particularly on its focus area of ‘ensuring equitable access’ to neurological care for all patients in need. These recommendations define our way forward and are a proactive framework for action. Ensuring that the EFNA work programme is consistent and capable of impacting policy discussions throughout the 2019-2024 EU mandate is essential in order to make progress in the areas identified.
Read the Position Paper here: https://www.efna.net/efna-publish-position-paper-on-access/


