
Oct 25, 2019
 “Stroke survivors in the UK are going without vital care and support. There are 1.2 million stroke survivors across the UK, but sadly 45% of people feel abandoned after leaving hospital” says Juliet Bouverie, Chief Executive of the Stroke Association UK.
“Stroke survivors in the UK are going without vital care and support. There are 1.2 million stroke survivors across the UK, but sadly 45% of people feel abandoned after leaving hospital” says Juliet Bouverie, Chief Executive of the Stroke Association UK.
SAFE: What is one issue related to the life after stroke in your country that you think needs special attention?
JB: We need to put the spotlight on long-term stroke care and rehabilitation. As anyone dedicated to helping stroke survivors rebuild their lives will recognise, the condition is extremely complex. People affected by stroke need rehabilitation that covers emotional support, help with finances, support services for carers, as well as physiotherapy, and speech and language therapy. Sadly, a recent Stroke Association survey of stroke survivors across the UK found that, in the aftermath of their stroke, only 18% of stroke survivors were confident that they would get enough support to make a good recovery. And 80% of stroke survivors told us they initially feared they would be sent to a care home.
Stroke causes a wide range of physical, communication, emotional and cognitive difficulties, and more than half of survivors report fatigue, memory and concentration difficulties, anxiety or low mood. Time and again we’ve seen thousands of people adapt to a new life after stroke. But it’s only possible with the right specialist support – and a ton of courage and determination. But the sad truth is that thousands of stroke survivors do not receive the support they need with their recovery when they leave hospital. There are huge regional variations in stroke support and care, which leaves stroke survivors at the mercy of a postcode lottery. On average, stroke survivors receive less than half the amount of rehabilitation recommended by national guidelines and many report feeling ‘abandoned’ after leaving hospital.
We know there are hospitals, stroke units and dedicated professionals leading the way for stroke care and support right across the UK. But too many stroke survivors are being let down because they aren’t given ongoing support to rebuild their lives. We want everyone affected by stroke to have the rehabilitation and long-term support they need, no matter where they live. No stroke survivor should be denied the chance to rebuild their life.
SAFE: What would be the solution, i.e. what is your organisation’s position regarding this issue?
JB: We know that the number of strokes is set to increase, and that too many stroke survivors aren’t getting access to the services they need to make their best possible recovery after they leave hospital. At the moment, we know there’s too much variation in the quality and coverage of care: too many of therapies recommended by clinical guidelines aren’t available across the country.
Stroke is also a hugely expensive condition, costing around £26bn a year across the UK. If we don’t act to roll out some of the actions we know can stop stroke before it strikes, save lives and prevent serious disability, the costs will spiral. We can’t afford not to act.
We want everyone affected by stroke to have access to the support they need and should expect, in line with national guidelines. That’s why we’re working across England, Scotland, Wales and Northern Ireland to support and drive changes which will improve the lives of people affected by stroke. In England, for example, we’re working closely with NHS England to deliver the Long Term Plan for the NHS, which includes the National Stroke Programme.
This Programme supports health and care services to make improvements from prevention and treatment right through to rehabilitation and long-term support after leaving hospital, including psychological support for stroke survivors. Our focus now is to ensure promised improvements are delivered.
SAFE: Please tell us more about your organisation.
JB: We’re here to support people to rebuild their lives after stroke. We believe everyone deserves to live the best life they can after stroke. We want to drive better outcomes in stroke prevention, treatment and lifelong support for everyone affected by stroke
We provide specialist support, fund critical research and campaign to make sure people affected by stroke get the very best care and support to rebuild their lives. The Stroke Association also offers vital support and information through our Stroke Helpline. My Stroke Guide is our online community of over 11,000 people affected by stroke, which many people said helps with their recovery.
Rebuilding lives after stroke is a team effort. It takes the determination of stroke survivors and carers, the generosity of supporters and the dedication of the healthcare and research communities to get there. We work hard to connect everyone in the stroke community so that people can live the best life possible after stroke. We have a number of stroke clubs and groups which provide essential long-term peer support to stroke survivors, carers, family and friends.
The Stroke Association’s campaign, Rebuilding Lives, aims to change perceptions about stroke, and reach more people who need support with their recovery. We hope the campaign, which includes TV advertising, will help us get our message out to people who need help and support, and raise awareness that it’s possible to rebuild lives after a stroke. To find out more, visit https://www.stroke.org.uk/rebuilding-lives

Oct 20, 2019
Author: Anna Tsiakiri, PhD, Psychologist from the Greek stroke support organisation, Hellenic Alliance for Stroke
This weekend, the Hellenic Alliance for Stroke in cooperation with the Hellenic Neurological Society, Postgraduate Program “Stroke” of Democritus University of Thrace, Hellenic Society of Cerebrovascular Diseases, Department of Educational and Social Policy of Macedonia University co-organized a two-day scientific event on 19th & 20th October 2019.

The scientific part of the event consisted of lectures from distinguished speakers specialised in Stroke, both in terms of medical care and rehabilitation.
The informative event, that was addressed to general public, aimed to provide useful information about preventing Stroke- how to recognize stroke symptoms, how we should react. A special tribute was made to stroke survivors.
The theatrical group of students of Democritus University has prepared a performance in order to raise awareness of stroke prevention, while HOPA/FAST heroes presented their great work in different parts of Greece.


Hellenic Alliance for Stroke presented their activities and the role of SAFE.
Finally, the event was closed with a Latin performance.


Oct 18, 2019

Chris Macey, Head of Advocacy for the Irish Heart Foundation
“The rate of death and permanent severe disability from stroke in Ireland has been reduced by more than 20% in the last decade. But hundreds of people are still dying every year when their lives could be saved. And thousands more are not receiving basic services that would enable them to make the most of life after stroke” says Chris Macey, Head of Advocacy for the Irish Heart Foundation and a SAFE Treasurer.
SAFE: What is one issue related to the life after stroke in your country that you think needs special attention?
CM: Irish stroke services compare well internationally in the vital early period after stroke occurs. But as soon as a person’s life is saved they typically start to regress through poor access to basic therapies in hospital. In therapy terms, patients then effectively walk off a cliff after they pass through the hospital gates – for most physiotherapy, speech and language or psychological services are grossly inadequate or non-existent unless they can afford to pay themselves.
As a result, more people than ever before are surviving stroke only for many to have their recoveries squandered by the failure to deliver the therapy services either in hospital or the community that will help rebuild their lives.
These services require upfront investment, but we do not need to spend more money on stroke. We just have to spend what we have in a different way. For example, our research showed that out of a direct cost of stroke to the Irish State of €557 million a year, up to €414 million was spent on nursing home care and less than €7 million on the community rehabilitation that can keep people in their own homes.
In other words the system starves vital acute and rehabilitation services of funding only then to spend huge amounts of money after the time patients can be helped most.
SAFE: What would be the solution, i.e. what is your organisation’s position regarding this issue?
CM: We need to recalibrate expenditure on stroke services in Ireland, through upfront investment in acute services and a much greater priority for community rehabilitation services.
The average onset of stroke here is at age 73 and because we will have 50% more 73-year-olds here within the next decade it is vital that we futureproof acute services, first by improving the standard of our stroke units – just one out of 28 fully meets ESO guidelines at present. We need around 200 extra therapists to meet current needs. We also need to invest in thrombectomy services that Irish doctors helped pioneer and to expand Early Supported Discharge (ESD) services that get patients home quicker and improve outcomes.
The development of ESD will also start to address the chronic deficits in terms of therapists working in the community where there are few champions at present for better services. In addition, we have helped to spearhead the development of community rehabilitation teams – working across neurological conditions – to continue therapies after ESD treatment has been completed. Their development in pilot locations and then nationally has to be speeded up however to address the huge unmet need among stroke survivors in the community.
More resources must also be provided to support stroke survivors living at home – the vast majority of stroke support in our country is provided by the Irish Heart Foundation without State assistance outside Dublin and the north west of the country.
SAFE: Please tell us more about your organisation.
CM: The Irish Heart Foundation is Ireland’s national charity fighting heart disease and stroke. Our main activities include:
• Provides information on heart health to the public and media
• Supports patients in managing heart disease and stroke
• Provides heart health programmes in schools and workplaces
• Co-ordinates the training of medics and the public in emergency lifesaving skills (CPR)
• Supports research, education and development in the medical profession
• Advocates for better patient treatment and services and for public health measures that protect and enhance cardiovascular health
We have been particularly effective in developing progressive public health policy in Ireland. We secured improvements to stroke services that have reduced mortality by 20% and permanent severe disability by more than a quarter in the last ten years.
We were a leader of the coalition that ensured Ireland became the first country in the world to ban smoking in the workplace that has saved a life a day in Ireland for 15 years since and that has reduced the youth smoking rate from 41% to 12%.
We also secured Ireland’s sugar sweetened drinks tax, along with restrictions on junk food marketing to children on TV and radio. In addition, we ensured that defibrillators are present on all flights into and out of Ireland and we helped secure major changes to the law to reduce the harm done by alcohol.

Oct 17, 2019
Leaders in atrial fibrillation and wearable technology to develop educational content around atrial fibrillation to help identify and support those at increased risk of stroke
Press Release | THURSDAY, OCTOBER 17, 2019
The Bristol-Myers Squibb-Pfizer Alliance and Fitbit today announced at the TIME 100 Health Summit in New York that they are working together to help drive timely diagnosis of atrial fibrillation (AFib) with the aim of improving earlier detection in individuals at increased risk of stroke. The BMS-Pfizer Alliance and Fitbit plan to collaborate on the development of educational content and guidance to support people at increased risk for AFib. Upon submission and U.S. Food and Drug Administration (FDA) clearance of the AFib detection software on Fitbit devices, the parties will aim to provide users with appropriate information to help encourage and inform discussions with their physicians.
“We’re in a new era of healthcare, where we’re not only focused on developing treatments but also looking at the potential of technology and data to help patients learn more about their health,” said Angela Hwang, Group President, Pfizer Biopharmaceuticals Group. “We are excited about wearables and how our work with BMS and Fitbit may potentially help patients and physicians detect and understand heart rhythm irregularities.”
AFib is the most common type of irregular heartbeat and is a significant risk factor for stroke.1,2 Approximately eight million people in the United States are projected to be affected by AFib in 2019.3 As the U.S. population ages, this number is expected to rise, as adults aged 65 and older are at an increased risk of developing the condition.3 Because AFib can be asymptomatic, it can often go undetected, and some studies suggest that more than 25 percent of people who have the condition find out after they have a stroke.(1,4)
“At Fitbit, we’re focused on making health more accessible and, through our efforts with the BMS-Pfizer Alliance, we have the potential to support earlier detection of atrial fibrillation, a potentially asymptomatic condition that affects millions of Americans,” said James Park, Co-founder and CEO of Fitbit. “With our continuous, 24/7 on-wrist health tracking capabilities, and our experience delivering personalized, engaging software and services, we believe we can develop content to help bridge the gaps that exist in atrial fibrillation detection, encouraging people to visit their doctor for a prompt diagnosis and potentially reduce their risk of stroke.”
Wearable technology has continued to become more integrated in the healthcare landscape(5) as people have recognized the value that 24/7 health tracking can have for people of any age or health status, including those at increased risk for specific conditions. Yet, those who use wearables to track their heart rhythm may lack the education or guidance on what to do with the data gathered from their device.6
“Too many people discover that they are suffering from atrial fibrillation only after experiencing a stroke. In fact, some studies suggest that this is true for more than 25 percent of people who have the condition,” said Joseph Eid, M.D., Head of Medical Affairs, Bristol-Myers Squibb. “These efforts with Fitbit exemplify not only our unwavering commitment to addressing the evolving needs of patients with atrial fibrillation, but also our dedication to advancing care by embracing technology as a part of routine clinical practice.”
Please continue reading here.
Image source: Fitbit.com
Oct 14, 2019
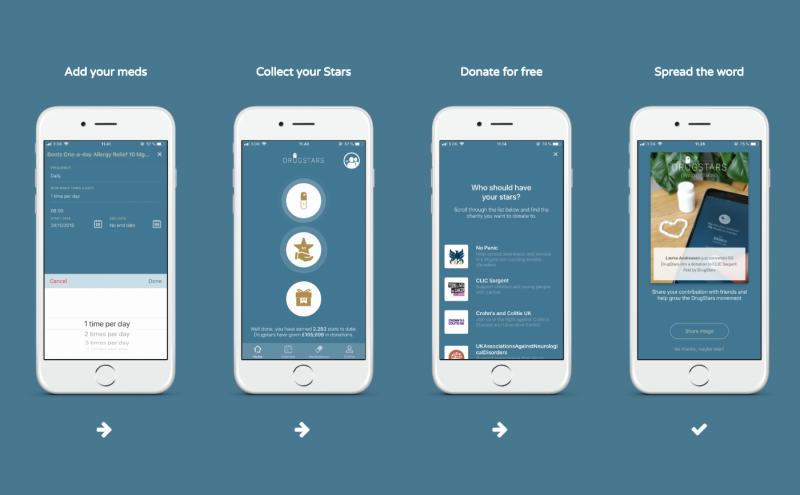
SAFE has joined DrugStars, a mobile application that enables you to make donations to your favorite charity just by taking your medicine as prescribed.
Drugstars ApS is a Danish company founded by Claus Møldrup, a former professor at the University of Copenhagen in modern medicine. He founded it together with Claes Rasmussen, former CEO at TWBA, Finn Overgaard, former CEO at RelationshusetGekko, Martin Plambek, former GM strategic marketing at Maersk Group, Jesper Kilbæk, former director of a bank, and Paul Clements, creative partner at Mensch.
Basically, DrugStars is an app that reminds you to take your medicine and awards you with stars that you can donate to health charities. But there is so much more in it: DrugStars hopes to become the largest patient movement in the world. A movement of patients who give to others just by taking their medicine as prescribed. And most importantly, a movement of patients who share their experiences and perspectives with regard to their medicines, so that this knowledge can be used to improve treatments. The ambition is to make you proud of taking your medicine the right way – to make you a real DrugStar.
It’s very simple to use DrugStars, and if you have any problems, don’t hesitate to ask by using contacts provided on their website.
How to start
First, you download the app and login with your Facebook account or create your very own DrugStars account.
Then, you register your medicine, vitamins etc.
You will receive reminders based on the information that you registered with your medication, and every time you receive a reminder, you will also be able to collect a ‘star’. You can also earn stars by reviewing your medicine or by referring other people to join DrugStars.
When you have earned 50 stars, you can donate them to one of the health charities in the app. DrugStars turns the ‘stars’ into real money and donates them to the health charities approx. every 6 months.
See some of the great memories in Donations.
If you wish, you can see a more detailed guide to the DrugStars app right here: Download The DrugStars Guide right here

Oct 11, 2019

Adam Siger, Fundacja Udaru Mózgu
“In Poland, we have access to all modern methods of treating stroke patients. We have a large network of stroke wards, where patients usually arrive quite quickly after the onset of a stroke. We are able to treat stroke in a modern way, but we have a problem all the time with proper care for the patient who usually leaves the stroke unit after 8 or 10 days” says Adam Siger, the President of the Polish stroke support organisation Fundacja Udaru Mózgu and former Board member of SAFE.
SAFE: What is one issue related to the life after stroke in your country that you think needs special attention?
AS: Access to specialist long-term rehabilitation is the biggest problem for people after a stroke, as well as their families and caregivers. we don’t have enough neurological rehabilitation departments. We don’t have enough caring and healing centers where we could accommodate the most difficult patients. We do not have a comprehensive support system for patients and their caregivers after leaving the hospital. Patients with aphasia as well as patients in the coma and in the persistent vegative state (PVS) are not usually admitted to neuro rehabilitation units. Similar problem applies to patients with swallowing disorders and nutrition by intranasal probes. Patients in such post-stroke problems will be left without proper support. A very big problem is access to complete rehabilitation after a stroke for the inhabitants of villages and small towns.
SAFE: What would be the solution, i.e. what is your organisation’s position regarding this issue?
AS: Since the beginning of our activity, our foundation has been undertaking a number of activities to increase the availability of modern rehabilitation and support for carers. We already have some small successes in this area but there is still a lot to do. We need to create a stroke national program for prophylaxis, treatment and rehabilitation. We believe that it is possible to consolidate the activities of many medical environments to create such a program. Every year, around 80,000 in Poland suffer from stroke. Stroke is a serious health problem but also social and economic. We hope that in the near future we will be able to interest politicians and decision-makers to create a working group in parliament that will deal with all problems related to stroke. We would like to interest politicians and decision-makers at the central and local levels to improve the situation of people after stroke
SAFE: Please tell us more about your organisation.
AS: Fundacja Udaru Mózgu is a non-governmental organization whose main goal is to help stroke patients, their families and carers. Our mission is all activities in the prevention, diagnosis and treatment of stroke. The Foundation’s activities also include prevention. Our publications on stroke, its effects and prevention are a valuable source of knowledge for the general public. We create social campaigns aimed at realizing the threat that this disease carries, using modern mass media.
We provide direct material and immaterial help to patients after stroke, their family and people with other neurological diseases. We run the only helpline in Poland for stroke patients and their carers.
We publish the Stroke Magazine “1 in 6” in Poland which we distribute for free at neurological departments and neurological rehabilitation throughout the country for free. The magazine is available for free on the Internet too www.magazynudarowy.pl
Thanks to the constant contact with patients from all over Poland, we know how important support and assistance is for people after a stroke.

Oct 10, 2019
 Kyiv, October 10, 2019– On the eve of World Stroke Day, representatives of the Ukrainian Parliament’s Committee on National Health, Medical Assistance and Health Insurance, National Health Service of Ukraine (NHSU), professionals providing Stroke Care to patients, and members of the public discussed what should be done by the state to ensure the availability of high-quality Stroke Care in order to reduce the mortality and disability from cerebrovascular disease.
Kyiv, October 10, 2019– On the eve of World Stroke Day, representatives of the Ukrainian Parliament’s Committee on National Health, Medical Assistance and Health Insurance, National Health Service of Ukraine (NHSU), professionals providing Stroke Care to patients, and members of the public discussed what should be done by the state to ensure the availability of high-quality Stroke Care in order to reduce the mortality and disability from cerebrovascular disease.
 The new Cabinet of Ministers of Ukraine, which has pledged to continue reforming the health care system, recently promulgated a Program where it set an ambitious goal of reducing the mortality rate by 5%. It is impossible to achieve this goal without creating a system of high-quality medical care for patients with acute stroke, as stroke is one of the leading causes of premature mortality and acquired disability in Ukraine.
The new Cabinet of Ministers of Ukraine, which has pledged to continue reforming the health care system, recently promulgated a Program where it set an ambitious goal of reducing the mortality rate by 5%. It is impossible to achieve this goal without creating a system of high-quality medical care for patients with acute stroke, as stroke is one of the leading causes of premature mortality and acquired disability in Ukraine.
In 2018-2019, Ukraine has taken the first steps towards creating a National Stroke Strategy. The Working Group, established by the order of the Ministry of Health (MOH) of Ukraine, has drafted the Stroke Action Plan in Ukraine for 2020-2030 and the Provisions on the network of healthcare facilities assisting patients with acute stroke specifying the requirements the hospitals are to meet. As of 2020, these services will be covered at the higher rates by the NHSU under the Guaranteed Medical Services Program. In addition, the MOH, together with the experts of the Working Group, collected information about the departments admitting acute stroke patients throughout the country. The experts were unanimous in that for our country the price of inactivity in this area far exceeds any costs of the right measures, any delay is unacceptable and it is to go ahead with the work started.

Prof. Mykola POLISHCHUK
“There are about 150,000 strokes every year in Ukraine. Many stroke patients are now being treated in general neurological or even therapeutic wards. This is unacceptable, and we request the local departments of health and hospital authorities change this situation as soon as possible, allowing stroke patients to be admitted only to specialised stroke wards. Research and real-world evidence in many countries around the world have shown that care provided in Stroke Units and Stroke Centers significantly reduces stroke mortality and morbidity as well as disability after stroke. According to the preliminary results of our data analysis, out of more than 500 wards admitting stroke patients in Ukraine, less than half have the necessary equipment for the diagnosis and treatment of stroke.
They are unable to perform the necessary workup and to carry out the necessary interventions. Up to 30-40% of stroke patients in Ukraine die within 1 month from the onset and less than 20% ever return to their previous level of daily activities. Our aim is to make sure that most of them reintegrate to the society and continue to live their life, ”- said Prof. Mykola POLISHCHUK, Neurosurgeon, the President of the NGO “Ukrainian Anti-Stroke Association”.

Dr. Maxim PEREBIYNIS
Dr. Maxim PEREBIYNIS, Subcommittee Chair, Ukrainian Parliament’s Committee on National Health, Medical Assistance and Health Insurance, answered the questions about the next steps the state needs to take in order to control stroke: “At the level of the Government, the Parliament and The President’s Office we are working to develop a program aimed at setting up a network of specialized stroke centers in Ukraine, with the involvement of the World Bank.
There are hospitals that already have trained doctors and necessary facilities, but many more are needed. However, a lot of work has yet to be done to properly plan the network of stroke centers, which should be located so that patients are delivered to the hospital on time (transportation should take less than 60 minutes).
To start with, it is necessary to analyze the existing institutions, technical and human resources in order to properly plan the network of these centers. Luckily, we don’t have to “reinvent a wheel”, we just need to implement what works well around the world. ”

Prof. Serhiy MOSKOVKO
Professor Serhiy MOSKOVKO, Neurologist, scientific adviser to Stroke Unit at Vinnytsia Oblast Psychoneurological Hospital, member of the Working Group under the MOH of Ukraine: The Working Group has drafted requirements for health care facilities that provide medical assistance for acute stroke. Compliance with these requirements demonstrates the hospital’s ability to provide high-quality stroke care. Overall, these requirements are an based on the requirements by the European Stroke Organisation adopted in many European countries. With institutions that meet these requirements, the NHSU will sign appropriate contracts in 2020 and will pay for the treatment of patients with stroke at an increased rate under the Guaranteed Medical Services Program.
We very much look forward to understanding and cooperating with the new team at the MOH of Ukraine. Our common goal is to make sure that every stroke patient in Ukraine has access to high-quality care and that hospitals that can provide such effective care have adequate supply for all the essentials, including alteplase, the drug for thrombolytic therapy. We need to significantly increase the number of thrombolyses in the country, then this will affect public health and mortality rates. For example, there are over 25,000 thrombolitic treatments performed in Poland per year compared with only 400 in Ukraine.

Mrs. Oksana MOVCHAN
Deputy Head of the NHSU Mrs. Oksana MOVCHAN told how the NHSU will fund the delivery of medical care to patients with acute stroke starting in April 2020: “In 2020 the tariff is going to be UAH 19,500 (about €720) per case. The tariff covers the workup for verification of the diagnosis, necessary care, medications from the National Essential Medicines List, excluding drugs provided through the government or local programs (such as thrombolytics), and acute rehabilitation. This tariff is almost three times as high as was paid under the medical subvention. We plan to arrange emergency medical services to deliver stroke patients only to those hospitals where they can receive timely and quality care.”
Mrs. MOVCHAN also emphasized that only hospitals that meet the requirements for acute stroke care will be able to receive payments from the NHSU at an increased rate. They are supposed to have all the necessary equipment and specialists to timely diagnose and treat stroke, in particular the equipment for neuroimaging: CT and / or MRI. The NHSU will not only pay for the service, but also monitor whether or not the hospitals comply with the terms and conditions of the contract. “In particular, this care package is absolutely free of charge for the patient, and hospitals cannot charge patients or families for this service,” Mrs Movchan said.
 Dr. Lyudmila LYPOVENKO, Head of the Neurological Department, the Second City Hospital in Bila Tserkva, shared her vision of the situation at the regional level: “As early as 2011, we began to perform systemic thrombolysis and have appreciated the difference between modern and old stroke care. In 2016, we set up a modern Stroke Unit with all the equipment and a multidisciplinary team. Now all stroke patients from Bila Tserkva and surrounding villages are referred to our hospital. A stroke patient who is a candidate for thrombolysis, bypasses the emergency department and goes directly to the CT scan, where the treatment is started immediately. We have done a lot to properly organise care pathways, however at times we are still facing a lack of thrombolytics provided by the state or local government. In 2019, we performed thrombolytic therapy in 55 patients, although according to the state program, we received the drug for only 10 cases. ”
Dr. Lyudmila LYPOVENKO, Head of the Neurological Department, the Second City Hospital in Bila Tserkva, shared her vision of the situation at the regional level: “As early as 2011, we began to perform systemic thrombolysis and have appreciated the difference between modern and old stroke care. In 2016, we set up a modern Stroke Unit with all the equipment and a multidisciplinary team. Now all stroke patients from Bila Tserkva and surrounding villages are referred to our hospital. A stroke patient who is a candidate for thrombolysis, bypasses the emergency department and goes directly to the CT scan, where the treatment is started immediately. We have done a lot to properly organise care pathways, however at times we are still facing a lack of thrombolytics provided by the state or local government. In 2019, we performed thrombolytic therapy in 55 patients, although according to the state program, we received the drug for only 10 cases. ”
Main Points:
• Every year, about 150,000 strokes occur in our Ukraine.
• Stroke and cerebrovascular disease are the second cause of death (more than 100,000 deaths per year or 13-15% of all deaths) and the leading cause of acquired disability in adults.
• Stroke mortality in Ukraine is several times higher than in Western Europe.
• High-qualitative stroke care is inaccessible, and 30-40% of stroke patients die within 1 month of onset.
• Stroke can strike at any age, and one third of stroke patients in Ukraine are people of working age.
• Ukraine has endorsed the European Stroke Action Plan for 2018-2030 and is moving towards a national stroke strategy aimed at reducing the burden of the disease.
 Thus, taking into account the Ukrainian Government’s Action Plan goal to reduce the mortality rate along with the epidemiological situation in Ukraine, we emphasize the urgent need to create in Ukraine a network of healthcare facilities that provide assistance to patients with acute stroke (120-150 Acute Stroke-Ready Hospitals or Stroke Units and 40-45 Stroke Centers).
Thus, taking into account the Ukrainian Government’s Action Plan goal to reduce the mortality rate along with the epidemiological situation in Ukraine, we emphasize the urgent need to create in Ukraine a network of healthcare facilities that provide assistance to patients with acute stroke (120-150 Acute Stroke-Ready Hospitals or Stroke Units and 40-45 Stroke Centers).
In order to provide high-quality care, timely imaging of the brain, its vessels and the heart as well as laboratory tests and evidence-based treatment, including IV thrombolytic therapy (if not contraindicated), should be guaranteed to all acute stroke patients.
This approach will reduce the burden of stroke for individuals, their families, local communities and the state as a whole.


Dr Marina GULIAIEVA, Ukrainian Anti-Stroke Association

Dr Dmytro LEBEDYNETS and Dr Mychilo Tonchev

Dr Yuriy FLOMIN, Ukrainian Anti-Stroke Association

Oct 9, 2019
First published on Imperial College London website
Written by Siobhan Markus
The European Researchers’ Night was an energetic festival of scientific exploration at the Natural History Museum (London) on the 27 September.
The Natural History Museum opened its doors after hours for a festival of scientific exploration called The European Researchers’ Night on 27th September. The tangled ‘world wild webs’ as went the theme of the night welcomed the public to interact with an eclectic mix of research and science from pop-up displays to one-on-one conversations over a pint in the ‘EU Pub’ and ‘Dialogue Den’. For the Research Project Management Office (RPM) at Imperial College London, it was the opportunity to bring four Horizon 2020 research projects EAVI2020, EDEN2020, PRESTIGE-AF and PERFORM2020 into the interconnectivity.
The delivery of these projects’ consortium, financial and communication management are coordinated by the RPM team and it was a no-brainer for the team to take these four projects, which are funded by the EU under the Horizon2020 program, and be part of the European Researchers’ Night. The projects’ scientists had a lot of fun showcasing their research in an interactive and engaging way and it was clear from public interest, the social impact that research fosters and is amplified through public outreach events such as this.
 The European Researchers’ Night is another EU-funded initiative, and Dr Marta Archanco, a project manager of the RPM team, explains that regular engagement in public outreach events is not only a funders’ requirement but it serves as a conduit in which scientists can express why their research matters while furthering the projects’ social impact. For this particular event, Marta says “what many people may not realise is that this event occurs simultaneously across Europe for one night of the year. Last year, during the 2018 Night, in cities across Europe over 1.5 million people were connected with science. This is a beautiful thing and we are so proud to have our Horizon2020 projects apart of this public event.”
The European Researchers’ Night is another EU-funded initiative, and Dr Marta Archanco, a project manager of the RPM team, explains that regular engagement in public outreach events is not only a funders’ requirement but it serves as a conduit in which scientists can express why their research matters while furthering the projects’ social impact. For this particular event, Marta says “what many people may not realise is that this event occurs simultaneously across Europe for one night of the year. Last year, during the 2018 Night, in cities across Europe over 1.5 million people were connected with science. This is a beautiful thing and we are so proud to have our Horizon2020 projects apart of this public event.”
Please read the full article here.

Oct 9, 2019
First published on ARNI Institute for Stroke Rehabilitation website
Loss of arm function is a very common problem after stroke. Put bluntly, if you have a stroke, it causes lasting damage to the part of your brain that controls movement in your arm. Stroke survivors may experience multiple upper limb symptoms resulting in complications such as weakness, planning and co-ordination problems, changes in the muscles (spasticity & flaccidity), subluxation, contracture, pain, swelling and a host of other symptoms and combinations of symptoms. The resulting presentation can render the upper limb virtually ‘non-functional’.
A well-known feature that can creep is called ‘learned non-use’, where the stroke survivor quickly gets very good at doing most reaching, grasping and releasing tasks with their less-affected, functional arm… ultimately him or her to forego efforts to improve the more-affected arm. Which is not good at all. Stroke survivors really want to know therefore whether intensive rehabilitation really does improve their upper limb motor control processes and reduce their impairments. And if it does, how should they go about getting this/doing it?
There is converging evidence that more therapy might result in better outcomes: current evidence suggests that intensive rehabilitation therapy helps people regain movement in their affected arm in the first few months after stroke. However, stroke survivors get to believe that little (if any) improvement can be made later on, which is sad, because we know this is not true.
Regaining lost movement may be possible many years after suffering a stroke, thanks to intensive rehabilitation therapy methods and inclusion of some principles, concepts and augments into rehab programmes, one of which is the use of robots. With the right therapy combinations, people can see improvements in movement, everyday function, and quality of life. Witness, for example, data which has emerged as a result of survivors attending the Queen Square (London) Upper Limb programme. See report in ACNR Journal. A majority improved in key clinical scores of motor impairment and arm function measured at admission and discharge and retain these improvements at 6-week and 6-month follow-up. Moreover, these are people improving months to years after their strokes occurred.
Is it the higher dosages of physical therapy/task-practice? Is it the combination of robotics and related augments alongside therapy/task-practice (therapy/task-practice aimed primarily at ramping up the dosage of repetitions on tasks)? For sure, as the RATULS Trial has emphasised, we need adequately powered dose-finding studies of promising interventions, tailored to targeted subgroups which also take into account potential cost-effectiveness to better understand the parameters involved.
Please read the full article here.

Oct 9, 2019
On October 4-6, 2019, the 5th National Congress with international participation of the Bulgarian Society of Neurosonology and Cerebral Hemodynamics was held in Sofia, Bulgaria.
 An excellent scientific meeting organized by Acad. Prof. Ekaterina Titianova, provided the opportunity to hear the latest update in stroke treatment and application of Neurosonology, exchange ideas and establish platform for mutual collaboration. The added value was the charming exhibition of the art work of stroke survivors and patients with other brain impairments, highlighting the importance of the life after stroke domain. It was a great example of joined forces of professionals and survivors in the fight against stroke.
An excellent scientific meeting organized by Acad. Prof. Ekaterina Titianova, provided the opportunity to hear the latest update in stroke treatment and application of Neurosonology, exchange ideas and establish platform for mutual collaboration. The added value was the charming exhibition of the art work of stroke survivors and patients with other brain impairments, highlighting the importance of the life after stroke domain. It was a great example of joined forces of professionals and survivors in the fight against stroke.
The congress was multidisciplinary and integrating the interests of different specialists – neurologists, neurosurgeons, angiologists, interventional specialists, etc. Over 180 delegates from Austria, Bulgaria, Israel, Italy, Republic of North Macedonia, Serbia and Spain, students in medicine, nursing, kinesitherapy, medical rehabilitation and ergotherapy from various medical universities, National Vasil Levski Sports Academy and universities in North Macedonia.

The forum was dedicated to the latest developments in ultrasound diagnostics of the nervous system with a focus on stroke, which continues to be the second cause of death in Bulgaria.
Within the international symposium Prof. Anita Arsovska from North Macedonia, who is also a SAFE Board member gave a presentation on “Optimal management of high risk asymptomatic carotid stenosis”.


