
Nov 27, 2019
In 2017, nearly 1.5 million people suffered a stroke, nine million Europeans lived with a stroke, and more than 430,000 people died due to a stroke in the 32 countries in a new study. The total annual costs for stroke were over €60 billion, a figure revealed by the Economic Impact of Stroke in Europe Report, funded by the Stroke Alliance for Europe (SAFE) and undertaken by a health economics team from the University of Oxford.
“We know stroke shatters lives. This latest evidence clearly demonstrates its ability to shatter entire economic systems if the business as usual approach continues” said Arlene Wilkie, SAFE Director General confirming the first part of the Economic Impact of Stroke in Europe report being published in the European Stroke Journal.
SAFE delegates at the Working Conference held in Porto today had an exclusive opportunity to hear first-hand about this research and its most important findings from Ramon Luengo Fernandes, research lead on behalf of the University of Oxford and Gary Randall, SAFE’s Research Manager and volunteer.
Ramon Luengo Fernandes, University of Oxford
The whole session with the presentation of the results was live tweeted and shared via SAFE Facebook.
Previously, in 2015, the overall cost of stroke for the European Union was estimated to be €45 billion. However, that study did not include nursing or residential care home costs, which may have biased the estimated costs of stroke downwards because evidence has shown that when a stroke happens, the survivor often needs to be placed in a specialised institution for further care, for example in a nursing home.

Gary Randall, SAFE Research Manager
This new study shows that with social care costs (nursing and residential care home costs), costs of productivity losses (the effect of sickness on person’s time off work; working years lost due to early death) and informal care costs (the time that relatives and friends spend providing unpaid care to people with stroke) being added, we have the first full overview of all stroke-related costs in all 32 countries in question. With this new information, the cost of stroke across 32 European countries is roughly 15 billion euros more than previously estimated in 2015. However, this is likely to be an underestimate, because some categories of healthcare costs, such as health education, public health activities, supportive treatments, home adaptations, and care provided outside the healthcare system were not recorded in healthcare statistics.
Further work commissioned by SAFE will estimate the number of people having, living and dying from stroke in 2030, 2035 and 2040, and how these changes will impact the economic costs of stroke across the 32 European countries in the study. These findings will be revealed in May 2020.
“The Economic Impact in Europe Report provides persuasive arguments for stroke to be considered as an investable proposition. We hope we have brought enough hard evidence for our partners, medics, researchers and policy decision makers to see the clear potential for investment in stroke prevention, treatment and life after stroke as a way for saving more lives and reducing future costs” concluded Arlene Wilkie.
This Report was made possible through educational grants from the following organisations: Boehringer Ingelheim, Amgen, Allm and the BMS-Pfizer Alliance.

Nov 22, 2019
Press Release | Source: EFNA
Launched in 2019, the #BrainLifeGoals campaign is raising awareness of the impact of neurological disorders by exploring the dreams and aspirations of those affected.
Sharing #LifeGoals has become a popular trend in social media. #LifeGoals are the often frivolous wishes people have – for example to own a designer handbag, meet a film star or drive a Maserati! Through this campaign people are putting a new spin on the trend by instead sharing their #BrainLifeGoals.
The campaign is an initiative of the European Federation of Neurological Associations (EFNA), an umbrella organisation representing pan-European neurology patient groups.
What are your #BrainLifeGoals for the New Year?
We’re approaching New Year- a time when it is traditional in many parts of the world to resolve to makes changes for the better, or to accomplish a personal goal. As part of the #BrainLifeGoals campaign EFNA is pleased to launch a photo competition on this theme. Participants are invited to submit photographs that reflect their goal for the future.
Get some tips on taking great photographs here.
Prizes
• The winning entry will receive a top prize of €500.
• Four runners-up will each receive a prize of €250.
Entries will be judged by a panel including patients representatives and professional photographers. Winners will be announced in late January 2020.
EFNA plans to hold an exhibition of entries at the European Parliament in Brussels during Brain Awareness Week (March) [to be confirmed], and again at the European Academy of Neurology Congress in Paris (May).
The competition will be open until Wednesday, January 1st 2020 at midnight CET.
CLICK HERE FOR ENTRY FORM.
COMPETITION RULES
• Photos should reflect the #BrainLifeGoals theme .
• Photos must be submitted via the entry form here.
• Photos should be high-resolution (a minimum of 1MB and a maximum of 6MB file-size).
• Photos may be taken using a regular camera, smartphone or tablet.
• Entrants must provide their name, nationality and email address.
• Each entry must be entirely the original work of the contestant, must have a title, description and indicate the location in which the photo was taken.
• Entries submitted in a language other than English should include English translation.
• Entrants should be personally affected by a neurological disorder.
• Any person included in a photo must have given their express permission to be photographed.
• By submitting a photograph to EFNA the contestant agrees to grant EFNA, free of charge, the right to publish the photograph online and in other EFNA media.
• The contestant agrees to grant EFNA the right to publish the name, nationality and entry details provided with their entry.
• Closing deadline for entries is 1st January 2020 and all entries must be submitted electronically.
• The winning entries shall be announced in late January 2020
• Entrants under 16 years of age, must obtain your parent’s or guardian’s permission before entering the competition.
• A maximum of three entries may be submitted by each participant.
• The judges’ decision is final and no correspondence shall be entered into.
• EFNA reserves the right to disqualify any entry which breaches any of these rules.
• An independent judging panel shall select the winner and runners up.
• All information submitted will be stored in accordance with EFNA’s Data Protection Policy.
Image source: EFNA
Disclaimer: This article was written by a third party. It does not necessarily express the views of the Stroke Alliance for Europe. The party who issues this press release is entirely responsible for the accuracy of its information.
Nov 15, 2019
PRESS RELEASE ¦ FRIDAY, NOVEMBER 15, 2019 9:00 AM EST
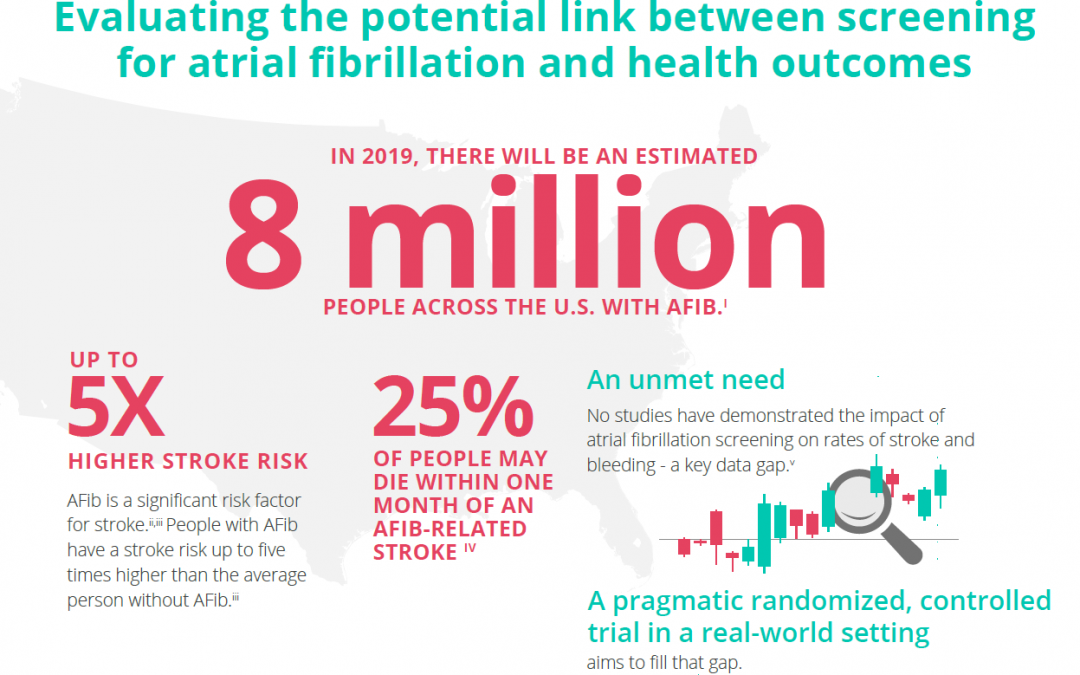
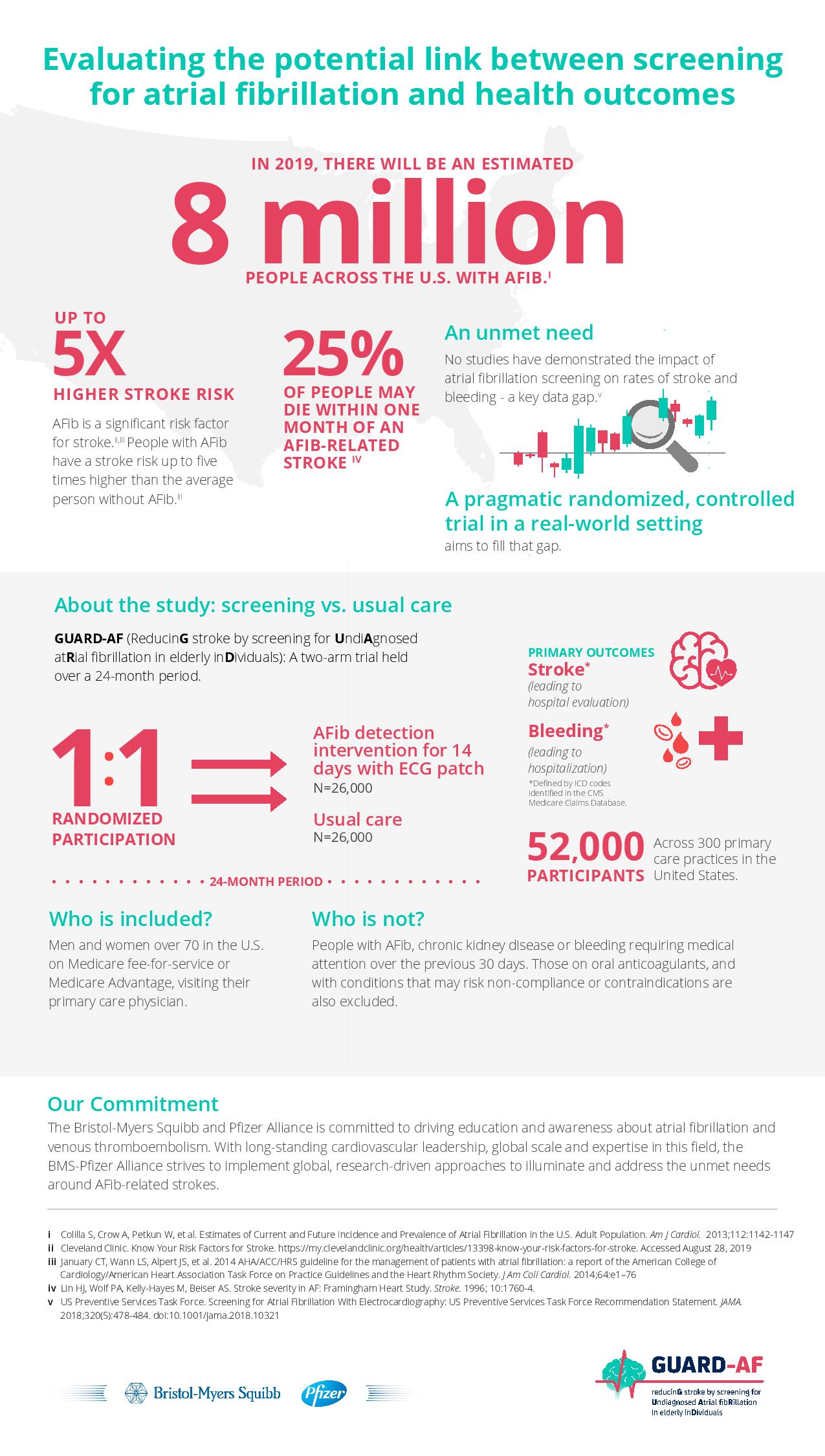
The Bristol-Myers Squibb-Pfizer Alliance today announced the initiation of a new randomized, controlled study, GUARD-AF (ReducinG stroke by screening for UndiAgnosed atRial fibrillation in elderly inDividuals). The study seeks to determine if earlier detection of atrial fibrillation (AFib) through screening in previously undiagnosed men and women at least 70 years of age in the U.S. ultimately impacts the rate of stroke, compared to usual standard medical care. This study will also assess potential bleeding leading to hospitalization, and therefore provide an evaluation of net clinical benefit or harm. AFib is the most common type of significant irregular heart rhythm, and it is estimated that 8 million people in the U.S. will be affected by AFib in 2019.i,ii AFib is a significant risk factor for stroke; stroke risk is up to five times higher in people with AFib than in those without it.iii,iv AFib can often go undetected, as it can be asymptomatic,i and some studies suggest that more than 25 percent of people who have an AFib-related stroke find out they have AFib after a stroke.v
“There is a real need for a study like GUARD-AF to assess the impact of screening for AFib on the crucially important outcome of stroke,” said Daniel Singer, M.D., Professor of Medicine at Harvard Medical School and Professor in the Department of Epidemiology at Harvard T.H. Chan School of Public Health, and an academic general internist at Massachusetts General Hospital. “This study has the potential to directly affect clinical practice and could lead to more AFib patients being identified and appropriately managed to avoid stroke.”
You can read the full press release here.
Disclaimer: This article was written by a third party. It does not necessarily express the views of the Stroke Alliance for Europe. The party who issues this press release is entirely responsible for the accuracy of its information.

Nov 14, 2019
Written by Alžbeta Husarovič, President of Porážka.sk
For this year’s World Stroke Day in Slovakia, a stroke support organisation Porážka.sk and a fashion stylist Andrej Kusalík organised a Charity Fashion Show. The event took place on 24th October 2019 in the Privee Lounge in Motešických Palace, in Bratislava, Slovakia.
 A successful Slovakian fashion designer Michael Kováčik created a T-shirt “Unbeaten” in three different outlooks for the Porážka.sk. These T-shirts were presented on a runway by Slovakian models and previous participants of the Miss Slovakia – Barbora Franeková, Magdaléna Šebestová, Eva Rezešová and Simona Brnová Slobodníková.
A successful Slovakian fashion designer Michael Kováčik created a T-shirt “Unbeaten” in three different outlooks for the Porážka.sk. These T-shirts were presented on a runway by Slovakian models and previous participants of the Miss Slovakia – Barbora Franeková, Magdaléna Šebestová, Eva Rezešová and Simona Brnová Slobodníková.
The main idea of the event was to auction money for the support of the Porážka.sk, with special focus on coveing treatment costs Peter Tatarko, an engineer who survived stroke in May 2018.
The main voice of the evening belonged one of TV moderators JOJ Lucia Wirthová. Apart from these designed T-shirts, the auction included a work of art by the academic painter Daniel Bidelnica and a painting by his wife Maria Bidelnicová as well. In addition to these two artworks also auctioned designer’s piece by Michael Kováčik, based on the auctioneer’s choice.
The evening was very successful and managed to auction around 6.500 EUR. The event was supported by leading bidders, celebrity photographer Petra Ficová, owner of Envy Lounge, Natalia Selveková and two anonymous auctioneers.
During the evening, the T-shirts were sold, bringing an additional sum of 800 EUR to Porážka.sk.
These beautifully designed T-shirts will continue to be sold on OZ Porážka.sk website www.porazka.sk, via Porazka.sk social media and on Zľavomat website, www.zlavomat.sk.

The funding that was generated through all of these activities will mainly be used for the treatment of Peter Tatarko, who overcame the defeat in May 2018. The treatment is expected to last for three intensive weeks. The cost of treatment is 3.500 EUR and Porážka.sk is very glad that it can help people through activities like this.
At the end, we would like to pass our massive thank you to everyone who participated and helped us raise the money. If you want to support our further work, please visit our website www.porazka.sk and purchase one of our beautiful T-shirts, knowing that you will not only get a very fashionable piece of clothing, but also help us continue with our very important work. Your purchase will be used for improvement of the lives of the stroke survivors in Slovakia.
A piece of the atmosphere at the event









Nov 14, 2019
Last month we were lucky enough to attend the Eye for Pharma Annual Patient Summit Europe in London. It was here that we also attended the first UK DrugStars patient organization event, where we proudly accepted a cheque for £500. This money was donated by UK patients using the DrugStars app.
DrugStars is an app, that helps you with your medicine. The app can help you remembering to take your medicine, but the truly special thing is that you also can donate money (FOR FREE) to patient organizations like us. So please download the app by this link https://drugstars.onelink.me/FN6p/83662720
#DrugStars #GivingByTaking #eyeforpharma #Patientsummit


