Apr 2, 2020
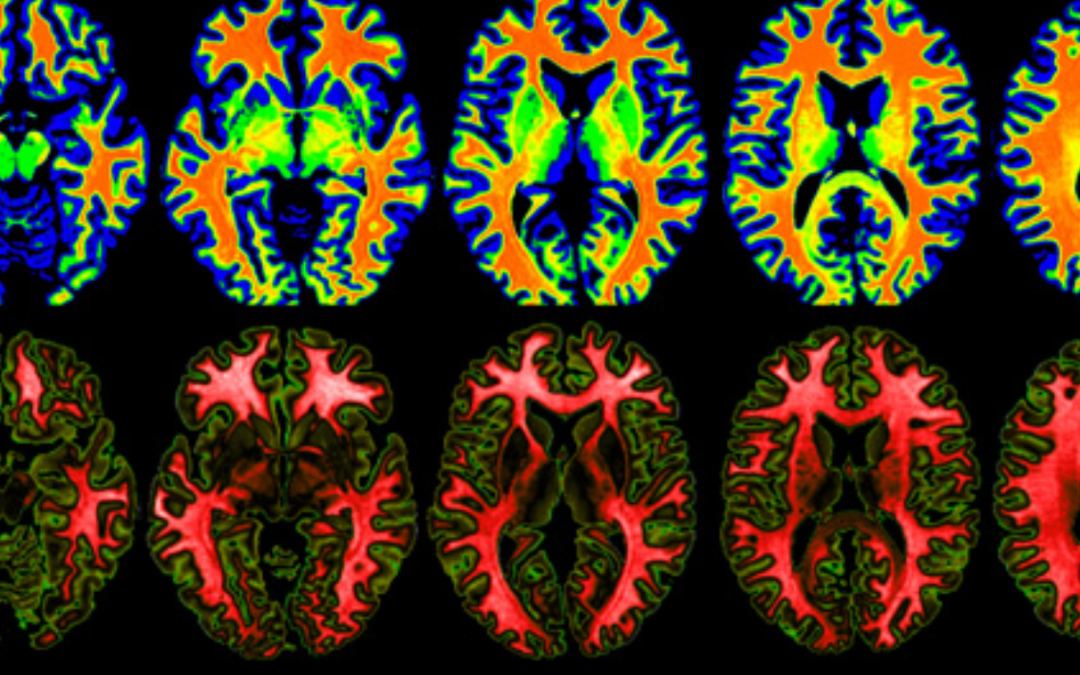
Damage to the small blood vessels in the brain (known as „Small Vessel Disease“) can lead to stroke and vascular dementia.
Despite causing these important conditions small vessel disease remains relatively poorly understood compared to other blood vessel diseases. With the better understanding of small vessel diseases, the study SVDs@target will develop novel therapeutic treatments and finally contribute to the prevention of stroke and dementia.
The project also includes 3 studies with stroke patients. They are:
ZOOM@SVDs, a high-resolution imaging study to look at vascular function and brain damage
INVESTIGATE-SVDs, an imaging study to assess the blood/brain barrier and vascular function,
TREAT-SVDs, testing the effects of different blood pressure lowering agents on vascular function in patients with distinct SVDs
Michael Stringer_UEDIN
We spoke with Michael Stringer, Research Fellow in Magnetic Resonance Imaging and Image Analysis from the Centre for Clinical Brain Sciences, Edinburgh Imaging and the UK Dementia Research Institute at the University of Edinburgh.
Why does this trial (Zoom/INVESTIGATE or TREAT) on small vessel diseases matter?
Investigate-SVDs recruits small vessel disease (SVD) patients to have advanced magnetic resonance imaging scans. SVD remains poorly understood, this study has great potential to further knowledge & ultimately improve outcomes for patients.
What is it that you do in this project?
As a research fellow in medical physics at the University of Edinburgh I helped setup the magnetic resonance imaging protocol (guide to running the scans), liase with other sites and am heavily involved with analysis of the imaging data.
Why do you do it?
My research focuses on applying advanced imaging and mathematical methods to study disease. I enjoy applying these tools to study real world problems, and as a highly multidisciplinary area it provides a lot of variety – it is seldom dull.
SVDs@target has received funding from the European Union’s Horizon 2020 research and innovation programme under grant agreement No 666881.
Photo credit: A print screen from the official SVDs@Target website.

Apr 2, 2020
The European Federation of Neurological Associations (EFNA) are pleased to publish a position paper on ‘Advocating for access to neurology treatment, services and support’. The document is based on feedback from an EFNA workshop held in Warsaw in October 2019, attended by approximately 50 representatives of patient and health professional organisations, industry partners and other experts. The contents of this paper reflect the insightful and lively debates and the arising conclusions and recommendations.
These outputs have been captured to inform EFNA’s strategic plan for 2020-2025, particularly on its focus area of ‘ensuring equitable access’ to neurological care for all patients in need. These recommendations define our way forward and are a proactive framework for action. Ensuring that the EFNA work programme is consistent and capable of impacting policy discussions throughout the 2019-2024 EU mandate is essential in order to make progress in the areas identified.
Read the Position Paper here: https://www.efna.net/efna-publish-position-paper-on-access/

Mar 30, 2020
Author: Jelena Misita, SAFE Awareness and Advocacy Manager
As we witness an unprecedented global public health crisis, many of us are forced to #stayhome for the greater good and stop Covid-19 from further spreading.
In these extraordinary times, there are groups of people who became even more vulnerable than they were. The stroke survivors and their loved ones for sure make one of these groups.
To be honest, the situation wasn’t good to begin with. There are around nine million stroke survivors currently living in Europe, with a support that is often undefined, fragmented or non-existent in majority of European countries, as shown in previous SAFE research projects, the Burden of Stroke Report (2017) and the Economic Impact of Stroke Report (2019).
Recent advancements in medicine enabled more lives to be saved in the acute phase of stroke, meaning that more and more stroke survivors will get a chance to live another 10, 20, 30 years or even longer. However, survivors and their families may face decades of existence in which they are largely reliant on self-management. The problems caused by stroke-related disabilities are often complicated by other diseases and additional issues related to their internal and external environment, self-care and self-esteem, their role as a spouse, parent, employee, and so on.
If you add the Covid-19 crisis and its implications to an already long list of difficulties that stroke survivors face every day- it may be just too much for them to handle. If whole hospitals are being turned to Covid-hospitals, what is happening with people who have a stroke? We learned that stroke doesn’t choose the time or place. It doesn’t discriminate and it can happen to anyone at any time, even in the Covid-19 most affected areas. Where does that leave the person who suffers a stroke? How likely would it be for this person to receive the necessary treatment in these conditions?
To get answers to these and many other questions, the European stroke community needs more skilled stroke advocates, who would be able and willing to take a stand and advocate for better stroke prevention, treatment and especially for better life after stroke conditions, because, as SAFE’s Board member and stroke survivor Grethe Lunde said, a saved life must also be lived.
If you feel it within you, if you want to make a change, but don’t know where to start- we have a solution for you. It is called SSOFT- the Stroke Support Organisation Faculty Tool.
SSOFT is a free platform. It provides knowledge and training on how to make effective advocacy activities and campaigns to deliver positive change at a local and national level on stroke prevention, treatment and care. This innovative eLearning platform includes six modules that provide information on:
Module 1: Stroke Support Organisations (SSOs)
Module 2: Making Change Happen
Module 3: Use of Evidence
Module 4: Role of Patient Voice
Module 5: Health System Advocacy
Module 6: Public Advocacy
In the end, why not using this period of isolation and social distancing to improve our skills and be better prepared for the changed world when the crisis is over?
We know that stroke survivors and their families will be thankful for it.
It’s up to you, click here, register and become one of us.

Mar 27, 2020
Source: World Stroke Organization
The Global Stroke Alliance Meeting, held in Rio de Janeiro, Brazil from March 11 to 14 was an innovative meeting that aimed to stimulate a global alliance to improve stroke care worldwide and to discuss the best strategies to implement evidence-based interventions access the continuum of care
 The Global Stroke Alliance Meeting brought together leaders from 20 countries around the world with extensive experience in the organization of stroke systems of care, alongside researchers, health professionals, health managers, scientific societies, private hospitals, industry and patients associations. There were 570 in person participants and several by teleconference, with live transmission from the main sessions. The meeting reached its goal of disseminating knowledge, exchanging experiences and creating action plans tailored to each region. All actors working together, joining initiatives and adding efforts in the same direction.
The Global Stroke Alliance Meeting brought together leaders from 20 countries around the world with extensive experience in the organization of stroke systems of care, alongside researchers, health professionals, health managers, scientific societies, private hospitals, industry and patients associations. There were 570 in person participants and several by teleconference, with live transmission from the main sessions. The meeting reached its goal of disseminating knowledge, exchanging experiences and creating action plans tailored to each region. All actors working together, joining initiatives and adding efforts in the same direction.
In addition to representatives of international stroke societies, several representatives of Ministry of Health of Brazil and Ministry of Latin American countries, Health Secretaries from States and Cities of Brazil, the meeting included a strong participation of Dr. Anselm Hennis, Director of Non-Communicable Diseases of Pan American Health Organization from Washington – that represents World Health Organization in Americas.
The dynamics of the event included a series of forums on the most diverse themes, in an attempt to cover all fronts related to the disease -research, political, logistical and educational.
You can read the full article here.
Image by Pete Linforth from Pixabay
Mar 26, 2020
In 2018, the European Federation of Neurological Associations (EFNA) conducted a survey of young people affected by neurological disorder, to assess the impact of these conditions on their lives. Stigma was identified as one of the biggest issues affecting respondents.
As a result, EFNA has decided to develop a new survey, delving deeper into this issue, exploring the areas where stigma is felt and the situations which give rise to it. By identifying these areas EFNA can focus attention where it is most required and move to develop strategies that will combat stigma.
This survey is open to anyone who is living with a neurological disorder, living in Europe. The survey is available in 8 languages and will remain open until June 15th 2020.
Access the survey at: https://www.efna.net/efna-launch-survey-on-stigma-and-neurological-disorder/


